
Blog
Revisiting Thyroid Eye Disease (another look at TED)

TED is not this patient’s real name but the acronym as described below. The rights to this photo belong to the company making the treatments described below and in this link: Tepezza
I see a number of patients with Thyroid Eye Disease (TED) as the bulging of the eyes causes high degrees of exposure and related dry eye disease issues. While traditional and advanced dry eye treatments can help with that aspect of this troubling disease, a recent treatment option emerged, called Tepezza. In an physician-spec ad (annotated by me in parenthesis) from a group called MDNB (mdnbupdate@mdnbupdate.com), about this drug:
“TEPEZZA® (teprotumumab‑trbw) has demonstrated proven efficacy for the treatment of TED in clinical studies.1‑3 To help gauge results, the Clinical Activity Score (CAS) is used as a diagnostic tool to identify the signs and symptoms of inflammation characteristic of TED. CAS is a 7‑point composite score, measuring spontaneous orbital pain (unprovoked pain behind and around the eye socket), gaze‑evoked orbital pain (pain caused by otherwise normal eye movements), eyelid swelling, eyelid erythema (redness), conjunctival redness, chemosis (swollen membranes over the white of the eyeball), and inflammation of caruncle or plica (swelling of the membranes at the inner corner of the eye). A lower score indicates fewer symptoms.4
The CAS is a composite score with equal weighting of a number of factors and may be required for treatment approval. However, the factors may not be of equal clinical weight to patients or to physicians treating those patients.
Select Important Safety Information:
TEPEZZA may cause infusion reactions. Infusion reactions have been reported in approximately 4% of patients treated with TEPEZZA. Reported infusion reactions have usually been mild or moderate in severity. Signs and symptoms may include transient increases in blood pressure, feeling hot, tachycardia, dyspnea, headache, and muscular pain.

Patient 2 before treatment
Pretreatment2
Proptosis (the degree of bulging eyes): 24 mm
Diplopia (double vision): 0
CAS: 5
Eyelid swelling
Eyelid erythema
Inflammation of caruncle/plica
Conjunctival redness
Chemosis

After treatment
Posttreatment (Week 24)2
Proptosis: 19 mm
Diplopia: 0
CAS: 1
Eyelid swelling

Patient 5 Before treatment
Pretreatment 5
Proptosis: 25 mm
Diplopia (double vision): 3
CAS: 5
Spontaneous orbital (eye socket) pain
Gaze-evoked (looking around) orbital pain
Conjunctival redness
Eyelid swelling
Eyelid erythema (redness)

After treatment
Posttreatment (Week 24) 5
Proptosis: 21 mm
Diplopia: 0
CAS: 0
No inflammatory signs and symptoms
Individual results may vary.
Both patients were treated with TEPEZZA in a clinical trial.
Both patients completed a full course (8 infusions) of treatment with TEPEZZA.
Both results shown are with no surgical intervention.
Help get your patient started on TEPEZZA
TEPEZZA is the first and only FDA‑approved treatment for Thyroid Eye Disease (TED)1,6, regardless of TED activity or duration. Review these steps for starting your appropriate patients on TEPEZZA here.”
_______________________________________________________________________________________
These results are compelling (while marketing will always showcase their best before and afters, I believe the majority of treated patients experience real results), so this sounds like really good news, and I think it is - as I mentioned in my earlier post on this topic here: https://www.eyethera.com/blog/8lemgnwt0bqqd15fmqr9ljrkdfe420. However, in various meetings I had with experts in San Francisco at the American Academy of Ophthalmology event 2 weeks ago, it appears that the effects are prone to “wearing off” - in as little as a year and a half. Retreatment can be done, and so far, appears to still be effective. Since it is such a novel and new medication, we are still learning about it – including (as I mentioned in my earlier post) its ability to cause permanent hearing loss in some individuals. Fortunately, this side effect appears relatively rare and monitoring hearing may give early clues that can lead to discontinuation before hearing is fully lost or steer us away from using this particular treatment in patients who already suffer from severe hearing loss.
One of the bigger problems is the cost, as a single course of typically 8 infusions can run into the hundreds of thousands of dollars (I heard as much as $340,000 from one expert and costs can vary greatly from region to region). This is mostly borne by insurance companies and is partly due to the cost of how it is given – requiring specialized staff to administer intravenous infusions (usually at “infusion centers”). The company is investigating allowing patients to give the medication below the skin in small injections - like a diabetic giving themselves insulin, as this method appears to be safe and effective in limited trials. Ultimately these costs filter down to everyone covered under these insurance policies, which can drive up costs for all – so I’m glad there may be a cost-effective alternative. Of interest was statements made by these experts that the age-old treatments, including oral steroids and radiation therapy, can offer similar benefits that appear to be more durable, so if Tepezza isn’t available to some, or eventually proves ineffective for many, then the older treatments are still likely to be of benefit. More encouraging was that a number of other “biologic” medications are being investigated for treating TED - which means more options may soon be available (and hopefully this will drive costs down and increase access).
From current clinical experience, many will be spared expensive, painful and potentially risky surgeries to decompress eyes by removing bone and the soft tissues swollen behind the eyes - by this new medication – so having a medical treatment that also avoids steroid and radiation side effects is still a very welcome addition to our medical treatment options!
To schedule an appointment with Dr. Jaccoma, call Excellent Vision at either of these two dry eye offices:
(1) 155 Griffin Rd, Portsmouth, NH 03801 (603) 574-2020
(2) 3 Woodland Rd, STE 112 Stoneham, MA 02180 (near Boston) (781) 321-6463
Testing Part 8 – Miscellaneous testing: the good, the bad and the ugly side of testing
The previous 7 parts of my testing series identifies some common testing strategies we employ – but is hardly comprehensive and really can’t be, since this field evolves almost daily.
It would be a stretch for every dry eye specialist to have every tool in the dry eye toolbox and the time to do every test, not to mention the cost, would be all-consuming. I’ll touch on some peripheral testing strategies and then speak to some of the common shortcomings we can run into. Good testing is when the tests lead us to a better understanding and then better treatment of a disease. Bad testing is when the tests can mislead us - and Ugly is what we get when we are lead down misleading, unnecessary “rabbit holes” - wasting time, resources and potentially harming our patients.
Patients who have “Pain without staining” are a special group – largely because pain is considered a subjective issue – but also because staining (with the stains mentioned in the earlier part of this series) can vary with something as simple as the weather (drier weather promoting more evaporation and dryness). But pain is a tough metric, mostly because doctors are still grasping at understanding the full gamut of pain – from the initiation of the sensation, up to the brain’s reception and interpretation of that signal. Unlocking this puzzle is getting a bit better understood and can start with a simple test - first of creating some degree of an uncomfortable event (touching the cornea with something that should register a degree of sensation – the cotton wisp, the fishing line, or some chemical such as increasingly stronger solutions of salty drops, or the common numbing drops that feel stingy before they numb).
Once we determine that there is the ability to sense some degree of “pain” at the surface, then we typically numb the eye with drops and see if the sensation of pain goes completely away. If it does, then this suggests something at the surface level and confocal microscopes are leading the way in showing swollen, inflamed nerves even when the surface “looks OK.” If the pain does not go completely away, then this implies a higher-level disorder – pointing to how certain pain centers in the brain can become amplified to where they can apparently “reverberate” or continue to signal pain (kind of like the thumb that throbs even when it appears to have recovered from a whack - you feel it, but you can’t see something wrong with it – at least unless and until it swells and turns hot and red). Sometimes all it takes to resolve this kind of pain is the therapy to make more and better tears - and to give it time to settle down – but sometimes time doesn’t heal it and it still hurts. This will be the focus of a future post as it is a complex and significant problem.
When the Schirmer’s is very low and we suspect Sjogren’s Disease (see my earlier posts on autoimmune disease, starting here: https://www.eyethera.com/blog/sjogrens-disease-autoimmune-dry-eye-part-1 ), the testing is imperfect at best. Hearing that the mouth (along with nose, throat, the GI tract and in women, the vagina) is extremely dry, along with the very low Schirmer’s, will often trigger a blood test and possibly a lip biopsy – but if everything is “negative” (and we’ve effectively ruled out other causes like certain medications and the common “anti-waters,” like too much caffeine and alcohol), then we may put a diagnosis like “clinical Sjogren’s” on it. Typically, I’ll treat it like Sjogren’s and have referred some to rheumatologists in case we missed something. Sometimes what was “negative” on lab testing may eventually turn “positive,” so this remains a bit of a “dark science.” Fortunately, there continues to be a lot of work in the medical field to help us find a better way to diagnose and treat these “autoimmune dry eye diseases.”
Because many metabolic, nutritional, and hormonal disorders can cause a constellation of health-related issues that include dry eye disease, it is often necessary to involve a larger group of specialists to sort this all out. Running wider batteries of lab testing can sometimes provide the necessary diagnostic clues to sort this out – and sometimes a good history can save a lot of lab testing – so history is key. Once we identify the prospect of associated diseases or metabolic imbalances, it is common to refer patients to the appropriate specialists in that field. Working as a team typically can afford patients the best outcome. As doctors continue to subspecialize in ever narrowing aspects of disease, we rely on them to teach less specialized doctors what they need to know to best serve their patients. These related subspecialties may include OB-GYN, Endocrine, Rheumatology, GI, ENT, Neurology, Dermatology and Allergy to name a few.
I can briefly touch on a couple of other common problems with testing and how I currently approach them:
- First, is the issue with Meibomography – covered in the first segment of this series on testing. It appears the InfraRed (IR) cameras commonly used to image Meibomian Glands are best able to show the “active” portions of the glands. This can make it hard to see portions of the glands that may still be present and otherwise healthy enough to “recover” their function. Patients and doctors can get overly nervous when presented with the pictures that show nearly (or wholly) absent gland tissue – yet on so-called “transillumination” the doctor may uncover substantial evidence of residual, less apparent gland presence. At least one Meibomography unit utilizes the combination of both direct-IR and transillumination technologies (Lipiview). Fortunately, a dark room, a slit-lamp (an eye doctor’s typical microscope) and a small flashlight can do a similar exam when paired with the IR photography – so a better idea of the likely level of recovery is available to most dry eye centers. Another issue with meibography is the inability to sort out the source of obstructions. Many times it is the common “waxy plugging” that may be visible at the level of the doctor’s microscope. Other times it may be from scaring or keratin plugs. (check out my earlier post on this here: https://www.eyethera.com/blog/why-do-expensive-dry-eye-treatments-fail-and-what-is-maskin-probing ) These are critical pieces of information, and technology-driven companies continue to innovate in this field – so more and better devices are continually coming into the dry eye specialist’s equipment marketplace.
- Second is the issue with drug interactions, medicamentosa and tachyphylaxis (a lot of confusing words!). Drug interactions seem self-explanatory, suggesting when two or more drugs react together, the sum of their effects (good or bad) can be amplified – or negated. The nature of their effects can turn in a fully new direction from the expected effect of either alone. As the field of medicine expands and the number of drugs continue to grow, this issue can (and does) quickly get out of hand. Computers and databases can (and do) help, and most pharmacies offer advice when their computers pick up the possibility of such interactions – but not all interactions can be known as some are uniquely dependent on a patient’s genetics and other disease states. Lastly, a drug interaction does not have to require another drug to “interact with” – as they can simply interact with the patient’s underlying genetic makeup or allergies to cause their unwanted effects. Using the history of which medications a patient is currently on as well as past history (especially anti-oil-gland medications like Accutane or some intentionally toxic medications like anti-cancer drugs), is necessary, since even relatively short courses of some medications can leave a long-term, dry eye imprint in their wake.
Medicamentosa is basically an unwanted reaction to a product, or the vehicle used to apply or carry the product. This product can be a single drug, cosmetic, preservative or even an “artificial tear,” where it causes an ill effect. It can also be an ill effect caused by a combination of drugs, cosmetics, preservatives or the oxidation caused by the interaction of air with the product (in or out of a bottle). This problem appears to be more common that I think most of us realize. One such example can be seen in glaucoma medications, where a single, or in some cases, multitude of drops - applied to reduce eye pressure, can “gang up” on the surface of the eye, causing redness and irritation. These drops can be necessary to prolong the quantity of vision but can reduce the quality of vision and therefore of life. Sometimes the problem is with the preservatives and sometimes it is the drug itself - or a combination, that causes this grief. It is up to the prescribing doctor to help sort this out and to hopefully find alternative ways that can be less toxic to the eye.
Tachyphylaxis is when the eye becomes “used to” a medication so that it requires more and more of that medicine to achieve a similar effect. Drops that cause blood vessels to squeeze (to reduce redness) are an example of this problem. As the drops wear off, the “rebound” of redness requires more frequent applications to get a similar effect (until even continuous applications may not be enough to reduce redness). See my earlier posting on this problem here: https://www.eyethera.com/blog/can-i-use-eye-whiteners-like-visine-or-lumify-when-my-eyes-get-red
The best way to resolve medicamentosa or tachyphylaxis issues varies, but we often have to require our patients to stop all medications, drops and products (never do this without the blessing of the prescribing doctors involved in your care) and then take a fresh inventory of the patient’s problems before adding them back. This is usually done by adding them back one at a time, to discover which are the more offending. Sometimes there are well known issues with medications and/or patterns of reactions that are immediately obvious to the dry eye specialist who can then more easily identify the likely culprit – so best to seek out a good one who can help in this regard.
To schedule an appointment with Dr. Jaccoma, call Excellent Vision at either of these two dry eye offices:
(1) 155 Griffin Rd, Portsmouth, NH 03801 (603) 574-2020
(2) 3 Woodland Rd, STE 112 Stoneham, MA 02180 (near Boston) (781) 321-6463
What do dry eye tests mean? (Part 7) Tear Volume (and how we measure it).
Probably the simplest test I do every day is – for me – one of the most important tests I consider in every dry eye evaluation. It has been around for over a century and involves a numbing drop and a tiny piece of filter paper placed along the edge of the eyelid for 5 minutes. It is called the Schirmer’s test and the reason I find it so useful is because it gives a reasonably accurate idea of the output of the “sprinkler system.” This helps to rapidly breakdown the source of dry eyes from one of two common pathways (that often intersect).
Simplistically, we can look at dry eye from the standpoint of tear quantity and tear quality. It can become very complicated when we look at what that means – but as dry eye doctors, we assess “Aqueous Tear Deficiency” or ATD and “Meibomian Gland Dysfunction” or MGD. ATD means not enough water and MGD means not enough (or not good enough) oil. This is important as treatments for one, generally are very different from the other. Since many patients have a degree of both, for simplicity’s sake, we might focus on the one that is the greater when the patient wants a stepwise approach (I like to advise tackling both simultaneously when clinically indicated and the patient is willing).
I have explained much of this in my earlier posts, and I always recommend that beginners go to the beginning of these posts to get updated. For regulars – or those in a hurry – I’ll point out that the “sprinklers” make the “good tears,” rich in water, salt, proteins, and oil (the “salad dressing”). The “emergency backup system” or “fire hose,” makes the salty tear water that floods the eye if it gets too dry, otherwise irritated, infected, damaged or if we emotionally cry. Numbing the eye helps to “turn off” this firehose reflex and allows the “sprinklers” a chance to do their job for the 5 quiet minutes we soak up that “salad dressing” tear.
Since most of this “good tear” (the “salad dressing” or “clear blood-like product”) is made of water, we can consider this the “Aqueous Tear” and too little leads to ATD. Fixing this nearly always involves drinking more water (to be fully hydrated). The obvious flip side is to also avoid too much “anti-water” (anything that encourages excess peeing – like caffeine, alcohol and many medications like antihistamines for allergies and sleep aides, decongestants for sinus congestion and cold pills, “water pills” for swelling and high blood pressure (check with your doctor prescribing these medicines to see if there are alternatives that would be safe for your health issues) – and the list goes on and on (bladder control pills, some mental health pills, high blood sugars as in less controlled diabetes, etc. etc.). After achieving a good water balance, the next step is reducing inflammation, as inflammation is particularly hard on the water producing cells involved with the Aqueous Tear production.
The number I like to see on this test is 15 millimeters or more – though patients under 30 years of age will often make 30mm or more, and the normal production levels tend to fall as we age. PRETTY MUCH EVERYONE SHOULD MAKE 10MMs OR MORE. This is because it takes about this much just to reasonably cover the surface of the eye (though more “open” eyes may need more - and less open eyes may get by with less). This helps understand how patients with excessively open eyes (like in Thyroid Eye Disease, or after “too good” a lid lift operation) can suffer even with “normal” tear amounts, as well as explaining why patients with droopy lids may tolerate relatively poor tear volume (and why a treatment for severely dry eyes can be the lateral tarsorrhaphy, where we surgically, partially close an eye for reducing exposure as added protection of the cornea). Punctal plugs may sometimes become indicated in this group (see my earlier posts on damming up the tears).
A common pitfall of this test is that it does require a careful attention to details to get a valid “number.” This involves making the surface sufficiently “numb,” (often harder to do when the surface has become overly sensitive from chronic dry eye damage and may require multiple drops), to turn off the “firehose” tear system. Then it is key to appropriately “dry” the gutter in the lower lid, to remove excess moisture (from the numbing drops and any patient-produced tears, so we can start from ground zero to measure only freshly made “sprinkler system” tears). Turning the room lights down also helps avoid glare-related reflex tearing and is better done early in this process. I start the “stopwatch” the moment I’ve finished drying this “gutter” (usually with a sterile QTip rolled gently along the floor of that “gutter”) and I’ve prepared the strips for placement at the start of the preparation for the test – so they are ready to go. A “Pro Tip” I learned, is to fold the outside edge of the strip for the right eye, so once placed and subsequently removed, it is easy to see which eye produced what result. Placement of the strips is along the outer (ear-side) edge of the lids so that the cornea is not directly impacted by these drying papers (avoiding extra stimulation of the firehose, as well as avoiding even minor damage to the cells on the cornea).
When the number is 6mm or less, it is sometimes not possible to effectively turn off the fire hose, as that has become the primary tear when the sprinklers are unable to produce enough tears. This is because the surface of the eye must stay moist to survive – when cells get dry, they die and drop off, exposing the underlying nerves and causing the pain these patients experience routinely. This is another “Achilles Heel” of the test – since we may get high numbers when we expect lower ones – but this can be inferred from other markers (like surface staining, tear salt levels and the microscopic evaluation of the tear layer along the lower lid if there is not too much conjunctivochalasis or CCH – as the “gasket effect” of that membrane can block the gutter-like reservoir in the lower lid from holding the normal volume of better tears and keeps the tear layer artificially high). It is also true that we will usually get similar numbers between the two eyes (unless one eye has had a unique problem, such as a single-eyed infection, injury, or surgery) – so if the two eyes have a similar history, we can usually expect a similar result on the test. When one is “abnormally high” when the other is “abnormally low” then it generally implies the higher one is artificially elevated by reflex tearing, and we go more by the lower one.
When the number is 10 or more (and we think this is a true reading), then we focus on the oil issues. Those patients should still stay well hydrated, since water levels can be quick to vary - and adding low volume to an otherwise poor tear oil is a recipe for ocular surface disasters. Making more and better oil generally requires eating good oil, doing good blinks, keeping that oil free flowing and keeping germs at bay, that would otherwise eat those oils and pollute those tears with byproducts of their digestion (What I call basic dry eye “Homework.”) Too much “germ poop” in the tears will lead to a vigorous immune response that can damage the tear glands and drive more ATD and MGD.
I’ve posted many times on our best tools for improving oils beyond this simple “Homework” – and this generally includes unclogging the oil (Meibomian) glands – with a heated expression - when the clogging is the typical, waxy plugs acquired early in this MGD disease (called evaporative dry eye). When they have been clogged for “too long” (which appears to vary by patient), there is a tendency to either develop “styes” (chalazia, as in an “acne pimple-like” cyst) or (more commonly) for the glands to silently wither and develop deeper levels of scarring that can “cut off” the glands. Scarring, if partial and mild, appears to respond to Intense Pulsed Light (IPL) and gentle, heated expressions. If the scars are more severe, then they often require probing (small, piano-wire-like tools used to “roto-rooter” the glands open). IPL also appears uniquely suited for stimulating the glands, reducing inflammation (by killing germs, mites and closing dilated blood vessels pouring the body’s “napalm, hand grenades and bazookas” into the tears, as a response to the irritation and damage caused by germ poop and dryness) and warming the glands to help in thinning the oils (though it doesn’t seem to keep the oil hot enough, long enough, to allow optimal expression – so I often advocate for following IPL treatments immediately, with an effective form of heated expressions).
Science is always looking for better tests - and a benchmark, century-old test is ripe for replacement by a “newer tool.” There is a test measuring “Lactoferrin levels” in tears, utilizing a tiny sample of tears, like the salt-level test. Lactoferrin is a common protein found uniquely in these “sprinkler system tears.” Low levels are more common in dry eyes and very low levels may indicate a higher risk of autoimmune dry eye (Sjogren’s being the usual one). It has been compared favorably to the Schirmer’s test and is now commercially available. Being relatively new, it remains to be seen how this will fit into the usual dry eye evaluation and cost remains an issue (the cost of a tiny piece of paper and a numbing drop is negligible and this newer test is not). I’ll keep you posted on this test as I develop some familiarity with it!
To schedule an appointment with Dr. Jaccoma, call Excellent Vision at either of these two dry eye offices:
(1) 155 Griffin Rd, Portsmouth, NH 03801 (603) 574-2020
(2) 3 Woodland Rd, STE 112 Stoneham, MA 02180 (near Boston) (781) 321-6463
What do dry eye tests mean? (Part 6) Inflammation (and how we measure it).
Inflammation is at the heart of dry eye disease. This is relatively obvious, as dryness causes irritation and irritation begets inflammation - fueling the vicious cycle of dryness and damage.

Red Right eye inflamed from glaucoma medications and dry eye disease - left eye had Durysta implant to reduce glaucoma medications - redness and dryness improved!
At the surface of the eye, inflammation causes redness, heat, swelling, pain and ultimately loss of function. The redness is a product of dilated blood vessels and the heat is a byproduct of increased blood flow. Dilated vessels carrying “defense products” from our immune system, will cause the vessels to get leaky - and the oozing of fluid through these leaky vessels causes swelling. The defense products (I like to refer to as “human napalm, handgrenades and bazookas” - but are really called cytokines, chemokines, antibodies and ultimately white blood cells) will put pressure on -and cause irritation to - the nerves around them (causing pain). This stimulates reflex tearing and leads to blurring vision - and may ultimately inflict damage to the eye’s surface. This warfare will affect the cells and glands that would make the “good tears” leading to increasing levels of salty tears and dryness - eventually damaging the cornea (or clear window of the eye - so loss of function). And this all relates to “common dry eye” - whereas autoimmune dry eye takes this to an entirely higher level (by adding ““human smart bombs” to the off-kilter immune defenses, aimed at the water producing glands - see my posts on this here: https://www.eyethera.com/blog/sjogrens-disease-autoimmune-dry-eye-part-1 through part 5 here: https://www.eyethera.com/blog/ogh4ia5gewpejt9cszlk0emeccuzh3
The “Need to know” has pushed science and technology to develop tests and time-tested methods to help detect and measure degrees of disease - and dry eye disease is no stranger to this need. The simplest method to detect inflammation is observation - looking for redness, heat, swelling, and surface damage. Pain is more subjective but the sense of irritation and pain is best tracked with validated questionnaires (see my first post on testing here: https://www.eyethera.com/blog/what-do-dry-eye-tests-mean ). Surface damage is commonly measured with staining dyes and excess salt levels quantitated in testing I’ve discussed in this same series. Some Keratographers (Oculus R-scan) allow more objective measurements of redness and thermal imaging cameras can provide information on heat elevations from inflammation.

Inflammadry Test kit (positive test indicated by pink stripe with blue control)
One of the newer tests for inflammation involves a rapid, in-office test that looks for a certain immune system “biomarker” that has been shown to be common to the dry eye pathway of inflammation, so-called “matrix metalloproteinase 9” (MMP-9). Quidel makes this test - called “Inflammadry” - and using a technique familiar to most, it looks like a “CoVid test” in terms of a blue control mark and a pink positive mark. Like the CoVid test, itis either positive (pink) or not (no pink) - so it is not a quantitative test (there is no gradient validated to measure the amount of MMP-9 in the tear - only that it meets or exceeds a certain amount considered abnormal). There is a Dacron spongy segment that needs to sit against the conjunctival membrane of the eye and “soak up” enough of a tear sample to give an accurate reading. The initial study report states: “As MMP-9 is a nonspecific marker, many conditions other than DE (Dry Eye) can produce a positive result. This information is found in the package insert and includes conditions such as recent ocular surgery, infection, or allergic conjunctivitis. The package insert further states that false negative results can occur in the setting of systemic immunomodulators, topical or oral steroids, cyclosporine, tetracycline, and topical azithromycin, all of which may inhibit metalloprotease activity. The test should be avoided in patients with cicatricial conditions that could lead to conjunctival injury or allergies to cornstarch, Dacron, topical anesthetic, or fluorescein dye.” https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5580996/
Because the majority of my dry eye patients have obvious amounts of inflammation and have eyes that are already uncomfortable from dryness, I’ve generally found this test to be more uncomfortable for the patient than the worth of reading a “positive” test (and if it’s negative, I’m not sure I always believe that, since many are already on some type of anti-inflammatory treatment and some are so dry it is hard to collect enough tear for a valid sample). Once a method becomes available to get a quick read on the amount of MMP-9 (hence the degree of inflammation present), then I’d be more inclined to want to measure that (especially if it was as easy and less irritating, as the salt testing I mentioned in the last post). Of interest to me, one of the more common pathways for MMP-9 to become elevated is for the salt levels to rise and “stress out” the cellular surface of the eye - so when the salt test shows high levels of salt, then a positive MMP-9 test can also be predicted.
More helpful, can be the Quidel test for the adenovirus common to causing pink eye (viral conjunctivitis). Since an eye can turn “pink” for a large number of reasons (including dry eyes and/or to many preserved drops like artificial tears or glaucoma medications - like my patient above) - and since this virus is extremely contagious, it can be useful to identify a viral cause when it exists (treating redness with a steroid makes sense when the redness is from dry eye-related causes, but using a steroid to treat a viral cause can allow the virus more time to evade the healthy immune response and cause the eye greater grief when the steroid is withdrawn). This test is also like a CoVid test (and a nasal swab for CoVid is often also indicated, since that virus is another highly contagious cause for pink eyes these days).
One of the reasons eyes can feel relatively “normal” even when many of our dry eye tests appear to show even severe levels of dry eye disease, has to do with corneal sensitivity. I touched on this point in my earlier blog post here: https://www.eyethera.com/blog/the-hill-of-sorrow-and-how-getting-better-can-sometimes-feel-like-getting-worse It is especially helpful to evaluate for reduced sensation of the eye’s (corneal) surface when we see this “disconnect” between how a patient reports they feel and how we think the eye probably should feel. A variety of tests are evolving to help detect and then quantitate this feeling - from as simple as asking if a patient feels a typically irritating drop when it is placed on the eye (and grading that response on a scale of 0-10), to testing with wisps of cotton, fragments of fishing line or pulses of air. Confocal microscopy (a special microscope that can scan the cornea with high magnification) can help detect abnormalities in the nerves that can help further explain such relative “numbness.” Fortunately we now have many tools to help bring nerves back (as nerves are important to the production of tears and serve as a necessary impulse to good blinking) - and the “Hill of Sorrow” post helps explain more about that, too!
To schedule an appointment with Dr. Jaccoma, call Excellent Vision at either of these two dry eye offices:
(1) 155 Griffin Rd, Portsmouth, NH 03801 (603) 574-2020
(2) 3 Woodland Rd, STE 112 Stoneham, MA 02180 (near Boston) (781) 321-6463
What do dry eye tests mean? (Part 5) Salt & why you don’t drink seawater.
As I noted in the prior testing segments, the Tear Break Up TIme (TBUT) is an indication of evaporation - and gets shorter (less time until evaporation) when the oil doesn’t “seal in” the water. The flip side of evaporation, is that only the water leaves - which means the stuff that is otherwise dissolved in that water remains behind. Since tears are salty by nature (and the fire hose is mostly salt water), the salt levels can climb quickly under conditions favorable to evaporation of tears. The ultimate conditions favoring evaporation are dry, windy air. Add to that, conditions that favor having eyes more open and you have a recipe for toxic levels of salt in the tears.
Salt levels are measured in terms of. “osmolarity” - a chemical term that quantifies the amount of salt in a solution. The higher the number, the more salt in that solution. Every cell in your body is subject to salt levels and blood carries a “normal” salt level of 275-295 “milliosmoles” of osmolarity. This is a reflection of the desired salt levels inside every cell in your body - and the surface cells on eyes are no different. Once salt levels rise above the level of salt inside the cells, water will seep across the cell’s border membranes in the direction of the salt, to “normalize” the salt on both sides of that membrane. As a result, cells “dehydrate” - becoming crinkled, shriveled up ghosts of themselves - before giving up the ghost completely. (Sorry, it is getting close to Halloween and ghosts must be on my mind).
Most know that if you get stranded at sea, the last thing you should do is drink the seawater, as it will only dry you out further and make you progressively more thirsty (until you get sick and die from thirst). Salt levels in tears can concentrate to levels higher than seawater and risk drying out the surface to toxic levels. Our “firehose” tears will become necessary to wash all that salt away - but those tears are not the “complete” tears from our “sprinklers” (which make water, salt, protein and oil) - so our surface gets progressively weaker, more damaged and drier.
Many dry eye specialists will measure salt levels with a tiny “bird-beak-like” device that dips into the tears lining your lower eyelid and “sips” a tiny amount of tears into the tip. A commercial unit found in many offices is the “TearLab” and their website offers additional information for those who wish to dive deeper (see the link below). Their device has a “test card” calibrated with a range of electrical elements that measure the flow of electricity across that salty water (higher salt levels conduct faster and better than lower) and gives a precise level of salt in the tears measured in those milliosmoles (mOsm/kg). Normal levels in tears range from 280-295, but once it climbs to 308 or more, it starts to become “toxic.” 316 -324 is “bad” but we commonly see levels higher than the salt-testing machine can register (it goes up to almost 400 and then becomes too high to measure). I find those with the highest levels to generally have the worst oil and faster evaporation (a TBUT generally less than 3 seconds and often less than 2 seconds).
Since TBUT is a good proxy for evaporation-related dryness (which is a proxy for poor oil), you might wonder why we would bother to also check tear salt-mOsm. Some patients have very active “fire hoses” which can largely keep up with salty elevations. Since each eye is separated on sides of the face and can have differing degrees of evaporation related to “which way the wind blows,” as well as having variable degrees of oils expressed with degrees of blinking, it is common to see wide swings in salt levels. When both eyes are very high, this can mean trouble with the fire hose keeping up and spell worse troubles for the surface trying to stay healthy. Even a difference of 8 mOm or more is considered significant, since salt is normally so carefully regulated by our eyes (and the consequences can be so great once salt levels get out of whack). High salt levels wreak havoc with the surface, causing burning, stinging, (reflex) tearing, blurring and scratchy sensations - basically every dry eye symptom since high salt leads to drier eyes. Some symptoms from other diseases can overlap with dry eye, so having more lab and clinical findings to help sort out the true causes can be a help.
Many patients ask if they can reduce their tear salt levels by avoiding salt in their diet. While this makes intuitive sense, it isn’t clinically true - again because of the innate, careful regulation of salt levels as part of our normal tear “recipe.” Just like blood is highly regulated, so too are our tears - and for the same reason - cells are delicate and salt levels are important. So the answer isn’t to reduce salt intake (at least for this purpose - check with your PCP if your blood pressure or other health issues might require you to alter the salt in your diet since a certain amount of salt is essential to your health). The better approach is usually to pay more attention to your oil intake and the function of the Meibomian Glands, that make the precious oils for your tears.
For a link to TearLab, see: https://www.tearlab.com/
To schedule an appointment with Dr. Jaccoma, call Excellent Vision at either of these two dry eye offices:
(1) 155 Griffin Rd, Portsmouth, NH 03801 (603) 574-2020
(2) 3 Woodland Rd, STE 112 Stoneham, MA 02180 (near Boston) (781) 321-6463
More on staining the surface of a dry eye and what it means…What do dry eye tests mean? (Part 4)
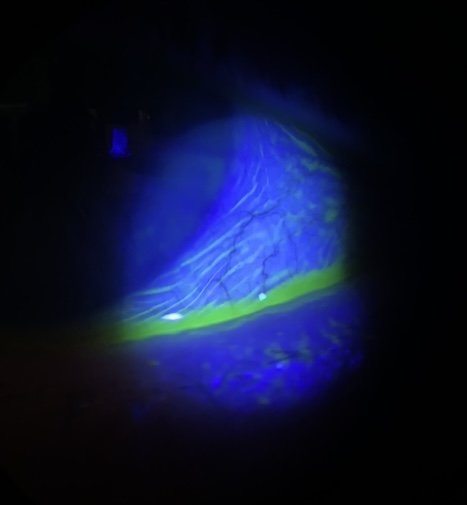
Last week I introduced the orange dye called Fluorescein and how it can color the tears in a way that allows dry eye specialists to monitor the “Tear Break Up Time” (TBUT). I mentioned it also stains dry, damaged cells on the surface of the cornea, so a dry eye doctor can assess the damage being done to the ocular surface by this dry and/or dysfunctional tear. This dye is a vital part of most eye exams and the amount, the timing from when applied to when examined and the dilution (and in what product - from anesthetics to salt water) can all have a bearing on how it stains and how it is perceived. There are patterns of uptake that are characteristic of certain eye diseases - so a skilled dry eye doctor has a lot to consider when interpreting how a dye like this reacts with their patient’s eyes. A blue light filter will help the orange dye “fluoresce” where the staining or puddling orange dye will now look bright yellow, to further highlight irregular and damaged areas on the surface of the eye.
Because a cell has to be significantly damaged in order for the dye to be absorbed into the cell (or to stain the footprint of where the cell used to live - but now is gone), the presence of any “staining” can be significant to the exam. Another common stain used to examine a dry eye is Lissamine Green and it is also non-toxic and generally well tolerated by the dry eye patient. It will stain more mildly damaged cells and is taken up by the conjunctiva more than the cornea (where Fluorescein is taken up more by the cornea and less by the conjunctiva), so is often used in conjunction with the orange dye when assessing damage from dry eye disease (which can affect the entire ocular surface). It doesn’t mix as well with anesthetics, but both can be easily diluted with salt water - and can be delivered in an unpreserved cocktail that should not damage any eye - but can give a better overall image of dry eye (amid other causes of) damage.
Where most areas of the body contain discrete focal points of immune fluid drainage and processing centers called lymph nodes, the eye strains and processes immune fluids through the conjunctiva first. Patterns of swelling in that otherwise clear, thin membrane can indicate various likely diseases which are differentiated into two main groups. Papillae are discrete round “bumps” with a small blood vessel at its core and are typically related to allergies and/or bacterial damage where Follicles are discrete round “bumps” of immune cells that push blood vessels away from the center. Fluorescein dye will “pool” around these bumps, highlighting them in a way that makes them more easily identifiable for the doctor to see. The conjunctiva on the underside of the eyelids tends to react more in this way and it is partly for this reason that a dry eye specialist (or any eye doctor) will often “flip over” eyelids (including the larger, upper lids) after applying some dye.
Friction in the area under the upper eyelid margin will cause a “callous-like” reaction (somewhat akin to the guitar-strummer’s thumb strumming the strings). The green dye will help light this up and it is further evidence of a dry eye (and especially of poor oil, since good oil would help lubricate that margin). Since the leading edge of the lid functions like a “windshield wiper” that helps distribute and replenish tears over the eye, the eye doctor term for this callous is “Lid Wiper Epitheliopathy” (or LWE for those in the know - and for more - see below). Friction over the white of the eyeball can lead to “Conjunctivochalasis” (or CCH) and the green dye can also light up zones around the pleats, folds and wrinkles of that now loose membrane while the orange-yellow dye can puddle along these folds (each uniquely highlighting that issue for the doctor to see). Dryness will damage the more exposed membranes and corneal surfaces first, so a pattern of yellow stippled staining over the cornea with the orange/yellow dye and green stippled staining over the conjunctiva will be more prominent in the average dry eye patient’s eyes.
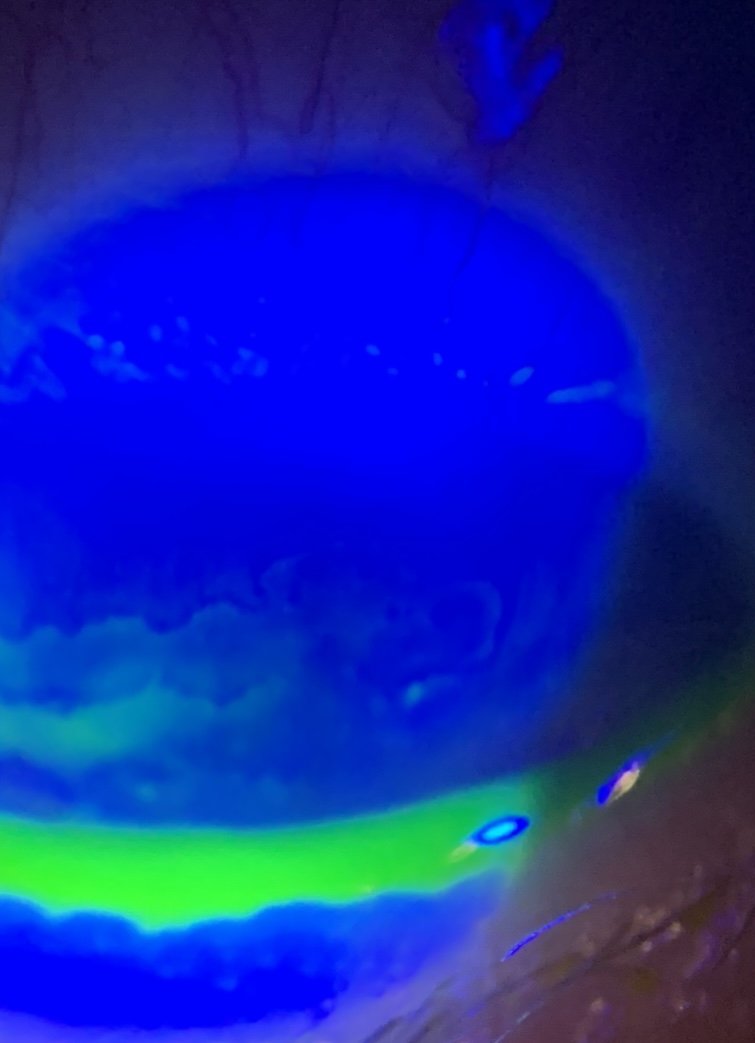
Fluorescein showing “reverse staining” over clear, raised areas of the cornea known as “Map Dot Fingerprint Dystrophy” (lower left side of image where dye pools around and under the irregular patches that don’t stain in this particular patient - see my link on this topic here: https://www.eyethera.com/blog/5b9vbda1r8e8r5y07l9bslgttcl4d8 as well as a few tiny dry spots (small bright yellow dots). The puddle of yellow-green is the tears lying along the lower eyelid margin that shows the typical irregularities or “notching” common to MGD.
My prior posts on CCH include some of the photos that show how the dye highlights the wrinkles of the otherwise invisible membrane like this one. For a quick link to more on this topic, click here: https://www.eyethera.com/blog/can-conjunctivochalasis-get-better-without-surgery
and here:

This illustration and to learn more at a doctor’s level about lid wiper, see this link: https://www.reviewofoptometry.com/article/lid-wiper-epitheliopathy-what-the-od-needs-to-know
To schedule an appointment with Dr. Jaccoma, call Excellent Vision at either of these two dry eye offices:
(1) 155 Griffin Rd, Portsmouth, NH 03801 (603) 574-2020
(2) 3 Woodland Rd, STE 112 Stoneham, MA 02180 (near Boston) (781) 321-6463
What do dry eye tests mean? (Part 3)
In most offices (including the offices of dry eye specialists), it is common to place a drop of orange (fluorescein) dye into each eye, in order to “see” the tears (now stained by the dye) and to see any “dry spots” (where dryness-damaged cells will take up the dye and show the degree of damage being done to the surface of the eye from a lack of good tears). Watching the dye become scattered by drying (evaporation) has been a standard method of judging the quality of a tear for generations (using the doctor’s slit lamp - or examining microscope) and is called a Tear Break Up Time (TBUT). The act of placing a drop of dye in the eye - with whatever “carrier” (some use anesthetic drops while other prefer saline) will “change” the results, because the drop alters the characteristics of the patient’s tear.
Many modern keratographers (instruments used in dry eye centers to investigate the causes of dry eyes) allow a so-called non-invasive tear break up time (NITBUT) measurement. This records the time it takes to see dry spots on the surface of the eye caused by evaporation and is not altered by drops, as it looks with projected light rings on the patient’s eye - to see “breaks” in the rings caused by evaporation (and runs a timer to see how long that takes from the time of a blink). This is considered a more “objective” test (not influenced by the attention span of the observing doctor) and is extremely useful in determining degrees of Meibomian Gland Dysfunction, because MGD means having less healthy oil floating on the surface of the tear. This oil will normally stabilize the tear by preventing evaporation (water has a hard time evaporating through an adequate amount of oil, akin to Saran Wrap sealing moisture from leaving a sealed container in the fridge). Without oil providing the “liquid Saran Wrap” function, comes rapid evaporation and dry spots. These dry spots function like little open sores on the surface of the eye, and are largely responsible for many of the classic dry eye symptoms - as salty tears will irritate these open sores, causing stinging, burning and reflex tearing.
Healthy tears commonly take 20 seconds or longer to begin evaporating (under standard humidity conditions). The “average” inter-blink-interval (the time between blinks) varies with the task and environment. The key driver of the blink reflex is when the cornea has a dry spot. When we are visually engaged (as in staring at computer screens), the brain can “override” the sense of a dry spot and allow considerably longer intervals between blinks (which can result in many dry spots that can interfere with vision and ultimately cause inflammation - as a response to irritation). Under in-office conditions, a “normal” blink interval can be closer to 10 seconds - so in my office we look for a NITBUT of 10 seconds or greater (meaning it should take 10 seconds or longer to see a single dry spot on a staring cornea) to indicate a good tear.

Courtesy of Topcon’s Brochure for their Topcon CA 800 Keratographer (used by the Excellent Vision Dry Eye and Rejuvenation Centers in Portsmouth, NH and Stoneham, MA). The red zones are the driest and fastest to dry - in as little as 3.4 seconds in the Left eye and 5.5 seconds in the Right eye for this “test patient.” Their “Interblink Interval” is 5.2 seconds - so potentially “keeping up” with the Right eye but not the Left’s rate of evaporation. These measurements indicate this patient does not have good tears - and is likely to have significant MGD as a cause of their dry eyes.
As I’ve stated before, a blink is the “heartbeat” of the eye’s surface. https://www.eyethera.com/blog/avoiding-a-heart-attack-on-the-surface-of-your-eye The interval between blinks is critical to maintaining a healthy surface, as frequent blinking can refresh that surface and prevent dry spots - as long as the interval between blinks keeps up with the evaporation and as long as the blinks are sufficiently strong and complete - to engage the oil glands and to fully turn over a tear. Some keratographers can assess that interval, as well as the time to acquire the dry spots - and can provide a graphic analysis that is easy to understand and to track over time.
Unfortunately, many factors can confound adequate measurement of the tear break up time, such as the humidity in the room (less humidity means tears will evaporate more easily into that dry air, vs more humid air), the force of the blink and ability of the blink to express oil from the glands, eye rubbing, recent artificial tears, air currents (fans or air conditioning) that provide fresh dry air to the eyes, and even the amount of germ activity along the lids with enzymes that turn oils into soaps. Even a lot of oil - if contaminated with these soapy residues - can quickly break down and allow rapid evaporation even when the oil otherwise seems fairly abundant. Lastly, some equipment is not up to the task of identifying very rapid blinks, and may continue to run the clock as the computer continues looking for evaporation. A rapid blink can keep the surface from otherwise evaporating, and therefore show a longer Tear Break Up Time (TBUT), than would be clinically true. Fortunately, the older technique of using the orange dye called fluorescein to stain the tears, and then to observe with a microscope during an eye exam can still be useful in identifying the more accurate tear break up time when the computer’s information appears suspect. Additionally, the foam is clearly evident during that exam.
A dry eye specialist will commonly look at computer driven data in the context of their own exam and the history from the patient, to best assess the condition of the Meibomian Glands and the amount and quality of oil they are producing.
To schedule an appointment with Dr. Jaccoma, call Excellent Vision at either of these two dry eye offices:
(1) 155 Griffin Rd, Portsmouth, NH 03801 (603) 574-2020
(2) 3 Woodland Rd, STE 112 Stoneham, MA 02180 (near Boston) (781) 321-6463
What do dry eye tests mean? (Part 2)
One of the reasons to seek out a dry eye specialist, is that to be a dry eye specialist, they should have invested time and money into obtaining and understanding up-to-date, specialty-specific technologies for diagnosing and treating dry eye disease. Thanks to the many engineers, companies and doctors leading the way – there are now MANY such technologies available and virtually no specialist will have (nor are likely to need) all of them.
If you wonder why many specialists charge what seem to be exorbitant prices for their services, it is worth noting that many of the diagnostic technologies cost upwards of $30,000 each and treatment devices can run $100,000 each - and the average clinic will have several such technologies. There are also the usual overhead costs of running such facilities and since inflation has gone up dramatically, hiring and keeping good staff who can run and service these machines, is at an all-time high. There is also a much-needed serious commitment on the part of the doctors (and their staff) to keep up with all of this technology, so in the end, it is never truer said, than: “you are likely to get what you pay for” in this field.
Now with that behind us, let’s get into the more specific dry eye exam.
In my center, perhaps the most useful device we use to examine and educate our patients with, is the so-called keratographer. This multi-functional machine allows us to image the Meibomian (oil) Glands in the eyelids, to monitor their function by determining the “Non-Invasive Tear Break-Up Time” (NITBUT), the “Inter-Blink Interval” (IBI), and to image the surface of the eye with diagnostic dyes (looking for dry spots, and the smoothness – or lack of smoothness – of that surface). It also can read the curvature of the cornea (useful in determining the power of focus of that part of the eye), to measure the volume of tear supported on the lower eyelid and to video the characteristics of the lids during the blink reflex. Some have software to create automated reports that can be used to relay information to the referring doctor or other specialists and may serve as a useful tool for the patient to keep track of their findings.
Imaging the oil glands is critical, as 85% of dry eye patients have a measure of Meibomian Gland Dysfunction (MGD) as a cause. The majority of these have visible abnormalities of these glands when photographed with InfraRed (IR) cameras such as those in the average keratographer. It is common to estimate the percentage of remaining gland tissue from these photos, though I find that IR photography tends to underestimate the amount of remaining tissue, as it appears to highlight only the active, oil-bearing portions (where a technique called transillumination can sometimes reveal what appears to be substantially more tissue). As these glands clog up, they tend to “constipate,” which causes them to dilate (presumably from increasing pressure trying to force their oils around the obstruction), and then to whither (atrophy). The eventual end-result is a loss of the glands and it can be difficult (if not impossible) to fully rejuvenate them with present technologies.
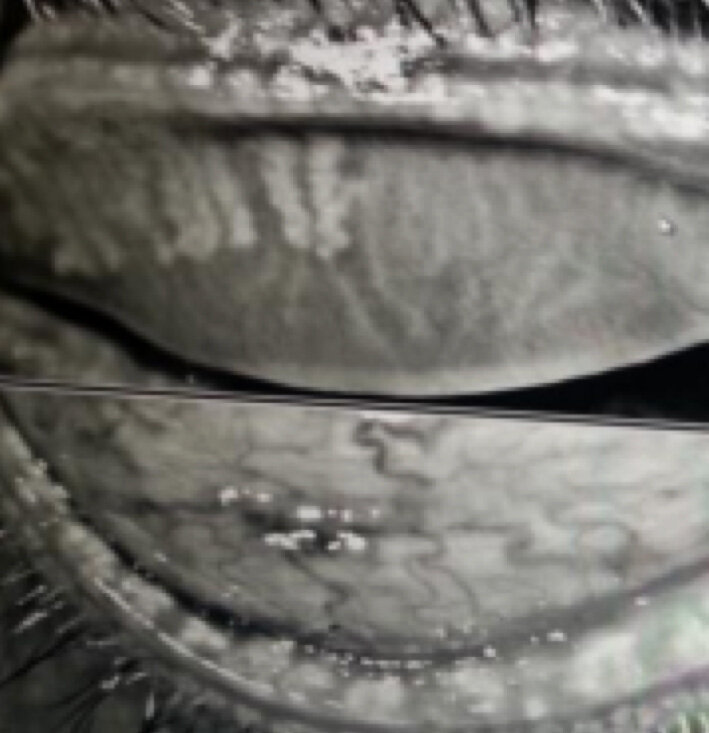
Meibomian Glands appear white, should run the full length of the rolled-over eyelid, and number 25-30 per lid. Most of these MGs are short, withered remnants - indicating an advanced degree of Meibomian Gland Dysfunction (MGD).
This photographic evidence is often alarming – both to the specialists and to their patients – and raises a significant “call to action.” It is hard to refute this level of evidence, even when symptoms and other clinical findings do not seem to appear quite as bad as this would otherwise suggest. What we’ve learned is that even as few as 6-functional glands per lid can provide sufficient oil so as provide a decent tear function. Because we are born with 25-30 glands per lid, this means we can lose up to 20-25 of them before we become aware we have a problem. Now that we are living longer lives, and using our eyes far more than previous generations would (given electricity to light our environments has only been common in households since the early 1900’s and power digital devices we use in all walks of life these days are common only in the last 30 years), it is incumbent on eye doctors to do everything in their power to ensure their patients have tear glands capable of lasting their patient’s lifetimes (and matching their lifestyle demands). I would have a hard time trusting a dry eye “specialist” to provide optimal care without the ability to image these glands. Next week, I’ll discuss some of the other functions of the keratographer and how we interpret these results!
What do dry eye tests mean?
Dry Eye is a complicated disease and testing can be complex and confusing. While I can’t interpret your specific tests, I can give a general idea of what tests mean. It is up to the dry eye specialist performing the tests to give the most accurate interpretation for each specific case.
That said, I will review some of the common tests you might find in a dry eye exam from a dry eye specialist. This list is not fully inclusive of all the tests a doctor might perform nor can I indicate every possible result.
History is perhaps the single most important diagnostic “test” we eye doctors (and really, virtually every doctor) have. Aside from determining the prior history, including any attempts to correct the dry eye problems, a validated questionnaire is very useful as it allows us to get a “number” relating to the degree of dry eye symptoms. While there are many such questionnaires, SPEED and OSDI are perhaps among the most common. Using “SPEED” (from https://eyewiki.aao.org/Dry_Eye_Syndrome_Questionnaires), Standard Patient Evaluation of Eye Dryness Questionnaire (SPEED)
“The SPEED questionnaire was designed by Korb and Blackie in order to quickly track the progression of dry eye symptoms over time.[9] This questionnaire gives a score from 0 to 28 that is the result of 8 items that assess frequency and severity of symptoms. The symptoms assessed include dryness, grittiness, scratchiness, irritation, burning, watering, soreness, and eye fatigue. The questionnaire further assesses whether these symptoms were not problematic, tolerable, uncomfortable, bothersome, or intolerable.[10] The questionnaire also monitored diurnal and symptoms changes over 3 months.[11] Validity of the questionnaire was determined by seeing how well it was able to segregate patients based on their symptoms, relative to the OSDI questionnaire (gold standard). The resulting sensitivity and specificity were 0.90 and 0.80 respectively.[11]”
A score of under 6 is considered minor but may still be associated with significant dry eye disease. The higher the number, the more symptomatic the individual. Because symptoms are so subjective, it is impossible to compare one patient’s symptoms to another. However, because the questionnaire is “validated.” It is likely that changes in a patients self-reported symptoms on this score will accurately reflect changes in their disease. We like to see progressive lowering of this score (indicating likely improvement).
Visual Acuity – probably one of the simplest and most underrated of dry eye tests. While 20/20 is considered “normal,” many eyes are capable of “better” - often as good as 20/15 (indicating what the average person can see at 15 feet, this eye can see at 20 feet). When eyes get dry, the surface gets irregular, and vision will suffer. When blinking affects vision (vision fluctuates with blinking), this is a common sign of dry eye disease. Checking for a glasses prescription is often an exercise in futility, as the variable surface gives variable results with almost every blink. A “Pinhole” is often employed to determine the best correctable vision, as this allows the patient to move the tiny hole over a more regular part of the eye, so vision can be optimal. If glasses are of a recent prescription and the pinhole still improves the vision further, this could be a sign of dry eye (or that the first prescription was incorrect). Other disease states (such as diabetes) can also result in fluctuating vision and an inaccurate prescription, so it is up to the doctor to determine the exact cause of blurry vision.
Another test common to most eye exams is most often included with dry eye exams – measuring IOP (IntraOcular Pressure). While a variety of technologies exist to do this, it is important to measure with the same technology each time as the results commonly vary between technologies but are validated within the same device. Average IOP is approximately 10-20 (or 22, depending on the group and the technology being used), measured in millimeters of mercury by convention. The reason this is important is that many times dry eye specialists rely on steroids to get inflammation under control – but steroids can lead to increased IOP and eventually, to glaucoma (the result of elevated IOP, resulting in damage to the nerve connecting our eyes with our brain). Losing that connection will result in permanent lose of vision (& ultimately to blindness).
I’ve blogged on the connection between dry eyes and glaucoma medications, so it should be obvious that patients on glaucoma medications are more prone to dry eye. What is also true, is that approximately 1 out of 10 average people placed on steroid eye drops will eventually (within weeks to months) have elevated IOP related to the steroids (the so-called “steroid responders”). Those with a tendency towards glaucoma (strong family history, and/or a tendency towards elevated IOPs and/or with “susceptible appearing nerves”), will have a likelihood of being a steroid responder as much as 1 out of 2 times. This means it is critical to monitor IOP when patients are being carried on topical steroids – to determine if they are a “steroid responder” and may progress to getting glaucoma. It is important to recognize that IOP is a relative number – and that some eyes may progress to severe glaucoma with IOP numbers that might be “normal” for others – where some patients may appear relatively immune to pressures that might normally cause glaucoma for others – so it is important to work closely with your eye doctors to determine what IOP is good for you.
More tests and interpretations coming next week!
Is it safe to buy an eye drop? “FDA issues warning letters to 8 companies for marketing unapproved eye products”
The recent news about people losing vision, eyes, and even lives from contaminated artificial tears already seems enough to convince us that “all eye drops are suspect.” This week’s FDA warning about 8 companies marketing “unapproved” eye products only heightens these concerns. Or does it? The good news is that - to my knowledge, no untowards injuries have been attributed to these products as yet. More good news is that the FDA is “on guard.,” as they should be - to protect us consumers from companies that don’t follow their rules (and their rules are strict for a good reason).
As most of you who follow my posts would know, my practice is devoted to keeping people safe - and helping them help keep their eyes in tip top shape. This means the bulk of what I do is to help my patients make more and better tears while ensuring the health of their ocular surface. In a perfect world, there would be no need for “artificial tears” (or related products) as everyone would have perfect tears. So my practice shyes from recommending artificial tears, as they can mask symptoms and allow patients who could make adequate tears if they worked at it. That “kicking the can down the road” without dealing with root causes, encourages the tear-making apparatus to stall and then to whither and go dry. Keeping that apparatus in good shape takes work - kind of like keeping teeth in good shape. And while we all appreciate eating, we tend to take vision for granted.
It is important to acknowledge that some - despite best efforts and for a variety of reasons beyond their control, simply cannot make a healthy tear in sufficient quantities, to keep the surface of their eyes healthy. And in today’s hard driving world of staring at screens all day, even the best tear producers may need a little help now and again. I therefore do recommend an “as needed” use of artificial tears and related products when it is necessary - but continue to push my patients (and readers) to work on making their best tears. My hat is off to the FDA and all of the people involved in keeping companies on track providing safe, effective products crucial to our health. The short story about these companies is here (and the full story from the FDA is in a link below that): From Healio:(https://www.healio.com/news/optometry/20230914/fda-issues-warning-letters-to-8-companies-for-marketing-unapproved-eye-products?utm_source=selligent&utm_medium=email&utm_campaign=news )
“September 14, 2023
1 min read
FDA issues warning letters to 8 companies for marketing unapproved eye products
The FDA has issued warning letters to eight companies for manufacturing or marketing unapproved ophthalmic drug products, the agency announced in a press release.
In an effort to protect U.S. consumers from potentially harmful eye products, the FDA addressed those that have been illegally marketed to treat conditions such as conjunctivitis, cataracts and glaucoma. Some of the warning letters also cited quality issues related to product sterility.
Eight companies received letters from the FDA that warn of legal action should they fail to correct violations for manufacturing and marketing unapproved ophthalmic products. Image: Adobe Stock.
The companies that received warning letters are Boiron, CVS Health, DR Vitamin Solutions, Natural Ophthalmics, OcluMed, Similasan AG/Similasan USA, TRP Company and Walgreens Boots Alliance.
“The FDA is committed to ensuring the medicines Americans take are safe, effective and of high quality,” Jill Furman, director of the Office of Compliance for the FDA’s Center for Drug Evaluation and Research, said in the release. “When we identify illegally marketed, unapproved drugs and lapses in drug quality that pose potential risks, the FDA works to notify the companies involved of the violations.”
The FDA requested that the companies respond within 15 days of receiving the letters and include a plan to correct the violations. Should the companies fail to comply, the FDA plans to pursue legal action, which may include product seizure and a court order to stop the manufacturing and distribution of an unapproved product. Some companies were also placed on import alert to keep their products from entering the U.S.
“We will continue to investigate potentially harmful eye products and work to ensure violative products stay off store shelves so that consumers can continue taking the medicines they need without concern,” Furman said in the release.”
The FDA link here for those who want the deeper dive:
Stay safe!
Can (CCH) Conjunctivochalasis (or anything to do with poor health) get better without surgery?
Maybe the better question is: How does our body repair itself and how can we assist it in that process?
General Wisdom is that our body turns over much of itself every 7-10 years. Corneal epithelium turns over every 2 weeks.
So it makes sense that outwardly irregular surfaces (or any disease state) can improve over time - assuming we take away the issues that drove it to “go bad” in the first place. I have seen degrees of improvement in CCH without surgery - the key is to start making enough quantity and quality of tears. With great tears, most symptoms of CCH improve (we see some patients with relatively severe CCH that have few if any related signs or symptoms). With poor tears, even mild to moderate degrees of CCH can become problematic and will tend to progress over time. This relates to the fact that plenty of good tears can wash easily over the eye with every blink - even with lots of pleats, folds and wrinkles in the conjunctiva (CCH). But with poor tears, those wrinkles really get in the way of the tears. Equally, if not more significant, the “gutter” or “reservoir” below the lower lid that is bordered by the eyeball, is shortened by the folds, so it can hold fewer tears.
My general push is to try every avenue that helps my patients make more and better tears before “fixing” the CCH (usually with the plications I’ve blogged on and published in my study). For more on CCH, see these earlier posts: https://www.eyethera.com/blog/what-is-conjunctival-chalasis-cch-and-why-should-i-care and for some embedded links to see how I actually do my treatments (and a study I published on the success of these treatments), see:
https://www.eyethera.com/blog/conjunctival-chalasis-cch-part-2-how-do-we-fix-it
Lastly:
https://www.eyethera.com/blog/cch-part-3-when-do-we-treat-cch-and-what-are-the-options
Healthy tears are also critical to healing the surface of the eye - so if, after working hard to improve the amount and quality of tears, the total volume is still suboptimal, then it often makes sense to fix the CCH, so that what a patient has for a tear, can better do its job.
Much research is being aimed at finding better ways to heal the surface when the tears are not up to the job. If the nerves are damaged (common in dry eye disease), then healing the nerves may be needed first. My earlier post on healing a “broken” surface of the eye is found here: https://www.eyethera.com/blog/what-to-do-when-the-surface-of-your-eye-gets-broken-scratched-operated-on-infected-or-otherwise-damaged A French study is underway to test another source of biologic material (Wharton’s Jelly - the material between the umbilical cord and the amnion) to heal poorly healing corneal surfaces: https://www.ophthalmologytimes.com/view/upcoming-trial-aims-to-measure-effectiveness-of-wharton-s-jelly-eye-drops-in-keratitis-treatment?utm_source=sfmc&utm_medium=email&utm_campaign=09062023_OT_eNL_Dry%20Eye%20house%20ad_CRU%20house%20ad&eKey=ZWphY2NvbWFAYW9sLmNvbQ==
For those interested in how the cells of the human body “turn over” every 7-10 years, I’ll first note the proviso that turnover does not mean we don’t age (seems obvious) - but it is pretty cool to understand the way our bodies work. This article helps explain how this works (or doesn’t work for some cells): https://www.livescience.com/33179-does-human-body-replace-cells-seven-years.html
More infectious eye drops and an FDA warning
The following is an article I’m adding to my series of bad eye drops. MSM is a controversial OTC product as there is a lot of online banter about reversing cataracts and other broad claims that have yet to have any adequate human trials to back up. Worse is when this comes in a contaminated eyedrop capable of possibly causing severe eye infections. Fortunately the FDA is blowing the whistle on this particular problem.
FDA warns against the use of certain illegally marketed methylsulfonylmethane (MSM) eye drops due to contamination
Aug 23, 2023
Martin David Harp
News
Article
The organization says to stop using Dr. Berne’s and LightEyez MSM drops immediately due to bacterial contamination, fungal contamination, or both.
(Image Credit: AdobeStock/Regina)
(Image Credit: AdobeStock/Regina)
The US Food and Drug Administration (FDA) is warning consumers to cease use and not purchase Dr. Berne’s MSM Drops 5% Solution and LightEyez MSM Eye Drops – Eye Repair due to bacterial contamination, fungal contamination, or both.
According to the FDA,1 using contaminated eye drops could result in a minor to serious vision-threatening infection which could possibly progress to a life-threatening infection.
While the FDA states they are unaware of any adverse event reports associated with the use of either product, patients who have signs or symptoms of eye infection after use should consult their health care professional immediately.
The Dr. Berne’s and LightEyez eye drop products contain methylsulfonylmethane (MSM) as an active ingredient. According to the FDA, these products are unapproved drugs and illegally marketed in the US. There are no legally marketed ophthalmic drugs that contain MSM as an active ingredient in the US.1
The FDA conducted sampling and testing based on the products’ intended use in the eyes, as well as because of the recent uptick in manufacturing issues with eye drops. According to the FDA, testing showed the products were contaminated with microbes and were not sterile.
Furthermore, the FDA identified bacillus bacterial contamination and exophiala fungal contamination in Dr. Berne’s MSM Drops. While the LightEyez MSM Eye Drops showed bacterial contamination from pseudomonas, mycobacterium, mycolicibacterium, and methylorubrum.1
According to the FDA, Dr. Berne agreed to a voluntary recall of their eye drops on August 21, 2023. While LightEyez Limited has not responded to the FDA’s request for a discussion over the concerns and has taken no action regarding a recall.1
References:
FDA warns consumers not to purchase or use certain methylsulfonylmethane (MSM) eye drops due to contamination. FDA. Press Release. August 22, 2023. Accessed August 23, 2023.https://www.fda.gov/drugs/drug-safety-and-availability/fda-warns-consumers-not-purchase-or-use-certain-methylsulfonylmethane-msm-eye-drops
This article comes from: https://www.ophthalmologytimes.com/view/fda-warns-against-the-use-of-certain-illegally-marketed-methylsulfonylmethane-msm-eye-drops-due-to-contamination?utm_source=sfmc&utm_medium=email&utm_campaign=08262023_OT_OYS-23-OPD0522_NOV-23-OPD0533_eNL_Oyster%20Point%20Dry%20Eye%20TRC_Novartis%20Viewpoints&eKey=ZWphY2NvbWFAYW9sLmNvbQ==
How Early In Life Can We Get Dry Eye Disease?
I often hear: “Isn’t my child too young to have dry eye disease?”
(or maybe, “Isn’t dry eye a disease of old people?” Most assuredly the answer is NO!
Dry eye disease appears to be on the rise and approaching a pandemic to match (or exceed) the Covid pandemic. Before writing this statement off as hyperbole, consider that the most common form of dry eye is evaporative in nature and caused by Meibomian Gland Dysfunction (MGD). A recent study (out of a tertiary care facility in India – though their observations match my mine, as well as many of my colleagues) showed that 95% of patients with clogged oil glands (obstructive MGD or o-MGD) have dry eye disease. Add to that, the fact that o-MGD is caused by lifestyle and dietary issues common to most Americans today, it comes as not surprise that more of us are affected – and at increasingly younger ages. Backing this up are several studies. One out of Duke University found that in nearly 100 children between the ages of 4-16 years (average age 10.5 years old), over half had some indication of MGD (yet few had any “symptoms.”) Another looked at high schoolers in Asia, where over half also had indication of MGD. Both of these studies were reported prior to the Covid pandemic (which appears another risk factor for dry eye – both from infections, from masks to avoid infections and from lifestyles associated with working and schooling from home on digital devices). I’ve published on two consecutive children referred for recurrent styes who had severe MGD, which was previously undiagnosed and not treated.
In earlier posts, I’ve explained the nature of these oil glands.
- First, they need basic building blocks of “good oil,” which are called “essential” because we can’t create them out of other oils. We need to eat them to make good oil for our tears (and as building blocks for every good oil in our bodies). These building blocks are called Omega 3, 6 and 9 and are generally best sourced in fish oil for the 3’s, tree nuts for the 6’s and seed oils for the 9’s.
- On top of eating them, we also need to digest and absorb them to nourish the oil glands in our eyelids (which in turn help support the clear, living surface of our eyes through our tears).
Two problems exist at this level.
- The first is that most Americans no longer subsist primarily on fish, nuts, and seeds (and perhaps like me, prefer pasta and pizza, hot dogs and hamburgers).
- The second is that many appear to have issues with digesting and absorbing what oils they do eat. This would be especially true of those with inflammatory intestinal issues, liver disease or gallbladder disease. While it is true that digestive issues are more common as we age, I see far too many young children dictating their menu and insisting on chicken tenders, mac and cheese, hot dogs, hamburgers, and pizza - to the exclusion of fish, nuts and seeds.
The next critical step is to “work” the oil glands, so they can produce their extremely important tear oils. These glands are composed of a series of tiny, sack-like balloons, lined by cells that produce the oils. The function of a strong blink is to “squeeze” these sacs and move the oil out of the balloons and into a common duct or passageway leading to the edge of the lid and then tiny, open “riverbeds” lining the lids, lead the oil to join our tears. The action of the lids spreading apart after full contact helps to drag the new, fresh oil and tear over the surface of the eye, while the action of the lids coming together with a slight squeeze helps to force the old tear down the passageway to the nose while simultaneously expressing the oil for the new tear.
Three problems exist at this level.
- The first is that too many of us are staring for long periods during the day (and night), while looking at our many digital devices. I’ve described this as the “ocular heart attack,” because a blink is both the “circulation” (turning over the lifeblood of our tears) and the impetus behind producing tear oils. No circulation of a tear is to the eye - like no circulation of our blood to our body (and the surface suffers). By not expressing oil, we are allowing the old unexpressed oils to “gel up” and by degree become more like candle wax than like the thin, “salad dressing oil” we need to float on top of our tear and seal it from evaporating.
- Second, we tend to do poor or “partial” blinks when we are engulfed in our digital world. This is a difficult concept for most, as we expect a blink to be a highly ingrained and automatic reflex (much like a heartbeat). But like a heartbeat, it can be weak or strong and when concentrating on our digital world (for work, communication, education, or play) we apparently “don’t want to miss anything.” Add that much of this digital experience happens when we are in a protected environment (house, office, school, or car), so there is less sunlight and wind to trigger the stronger blink responses. Remember to “blink strong.”
- Third, this stagnant oil sitting in our glands becomes better food for germs. These germs eating our tear oils will trigger our immune responses into inflammation (which can turn our eyes red and damage the cells making the watery portion of our tears). They also produce a gummy “biofilm” that – on our teeth we call plaque, but on our eyelids, we call “scurf.” This gummy plaque can “dam up” the riverbeds that would join the oil gland produce with our tears as well as to eventually cap over the oil glands and seal them. Waxy oils will further obstruct them and then you have obstructive MGD (and dry eyes).
Since all who develop o-MGD (and related dry eye) tend to do so slowly, over many months and years, it is common to “adapt” so that we can continue to function. Early on, we can increase our blink rate, to better keep up with the evaporation happening faster as we have less oil to seal the moisture in and dry air out. Normal blink rates average every 10-20 seconds, with longer periods between blinks when we concentrate (like when we stare at digital devices). Normal evaporation rates occur over 20 seconds or more (depending on the air dryness and general air quality). Blinking every few seconds is common (but also like running a marathon all day) when our oil is insufficient to seal and protect our tears from evaporation. Another adaptation is for the corneal nerves to gradually become “numb” (through various anatomic and physiologic responses). As children develop, they are good at adapting – but also tend to live in the moment as their collective recall of a distant past (when eyes felt and performed better) is limited by their age. Older adults who have experienced a youth of good eye health and tear function appear more apt to understand when this has “gone wrong.” For kids, the symptoms may be masked, or show up as recurrent styes or as under performance at schoolwork – or acting out when they don’t feel good but don’t understand what is wrong.
My earlier posts help to direct us to finding good sources for the essential omega oils 3, 6 and 9, as well as simple “lid crunches” coupled with warm moist compresses and lid hygiene. I’ve found that most younger patients (especially school-aged kids) will quickly respond to these simple steps and generally don’t require the more expensive and procedural approaches of my adult protocols (typically involving mechanical lid hygiene, IPL and RF-heated expressions of clogged MGs).
If In doubt about whether you or your children have dry eye disease, it is best to seek the examination and advice of a dry eye specialist who has the equipment and education to determine the health of the ocular surface and the tears that support that surface. I no longer treat children, but am happy to examine and treat adults and may be able to offer advice regarding their children.
To schedule an appointment with Dr. Jaccoma, call Excellent Vision at either of these two dry eye offices:
(1) 155 Griffin Rd, Portsmouth, NH 03801 (603) 574-2020
(2) 3 Woodland Rd, STE 112 Stoneham, MA 02180 (near Boston) (781) 321-6463
(July 23rd’s post includes an index to past posts which will not include this post but is otherwise a complete reference!)
Ophthalmologists: Castor oil shouldn’t be rubbed in the eyes, no matter what they do on TikTok (and more).
Reposted from Ophthalmology Times, Aug 8, 2023, author David Hutton
This first segment is reposted from: Ophthalmology Times, Aug 8, 2023 by David Hutton
(from: https://www.ophthalmologytimes.com/view/ophthalmologists-castor-oil-shouldn-t-be-rubbed-in-the-eyes-no-matter-what-they-do-on-tiktok)
Followed by my observations and a post regarding eyelash growth serum made from Castor Oil (see below) -
“Ophthalmologists are issuing a warning not to use castor oil as a way to treat vision problems amid claims circulating on TikTok.
In its heyday, castor oil was considered a jack-of-all-trades home remedy, used as a laxative, a moisturizer and even as a chest rub to ease lung congestion. Now, it is making a comeback as some influencers on TikTok claim they are using castor oil as treatment for vision problems.
However, ophthalmologists are sounding the alarm, according to an NBC News report, with dozens of videos on the social media platform receiving millions of views showing people rubbing castor oil over their eyelids, across their eyelashes and under their eyes to help treat issues like dryness, floaters, cataracts, poor vision, and even glaucoma.
Castor oil is a type of vegetable oil extracted from the seeds of the castor bean plant, and it has been used for thousands of years in traditional and folk medicine to treat a range of issues from bronchitis to skin infections.
It's considered safe to take as a laxative, but because of potentially severe side effects like vomiting and dizziness, castor oil isn't widely used anymore.
Despite warnings, TikTokers still promote it. One woman claimed that after two weeks of use, she doesn't need to wear reading glasses as often, while another said it prevented an eye infection from progressing.
Castor oil on store shelves are not meant to be used on the eyes and could contain dyes, preservatives, fragrances or other ingredients that can cause irritation or infection. It also may not be sterilized.
Limited research involving small sample sizes and no control groups have found eye drops formulated with a low concentration castor oil mixture helped with dry eyes and blepharitis, or inflammation of the eyelids, but experts warned of the low quality of the research, according to the report.
“We just can’t make a recommendation for something that has very little evidence behind it,” said Ashley Brissette, MD, MSc, FRCSC, a spokesperson for the American Academy of Ophthalmology and assistant professor at Weill Cornell Medicine in New York, said in a statement. “Castor oil is not a cure-all. If you have concerns about your eyes, you need to see an ophthalmologist.”
Castor oil does make a great moisturizer though, Brissette said. It contains ricinoleic acid — a type of fatty acid that prevents water loss through the skin — a reason why it's found in soaps, cosmetics, and lotions.
Moreover, Vicki Chan, MD, a practicing ophthalmologist in Los Angeles, said in a statement that castor oil does not have any effect on cataracts or glaucoma.
“These conditions occur inside the eyeball,” Chan said, “so even if you put a drop of castor oil on your eye, it’s not going to seep in and dissolve or fix anything.””
As a dry eye clinician, I (Dr. Jaccoma), will add that Restasis is 0.05% Cyclosporine A in a Castor Oil emulsion (tiny droplets of Castor Oil blended into water so that the oil stays suspended in the tiny droplet form). Since this is “PURE” CASTOR OIL - WHICH HAS BEEN STERILIZED - if is safe to apply it directly to eyes. Alone, (without the Cyclosporine A), it was initially also marketed as a Preservative Free artificial tear (the emulsion was called “Endura” and was carefully created to act as an effective transport for the cyclosporine medication). This means the Endura “carrier” was considered an effective artificial tear independent of the medicated (Restasis) version - so yes, certain forms of Castor Oil can be useful as an artificial tear. What is crucial from my perspective, is that “Based on review of the literature, the major lipids present in meibum are …waxes, sterols, and sterol esters, followed by triacylglycerides and fatty acids…Thus, meibum is a complex mixture of lipid molecules.” (From Wojtowicz JC, Butovich IA, McCulley JP. Historical brief on composition of human meibum lipids. Ocul Surf. 2009 Jul;7(3):145-53. doi: 10.1016/s1542-0124(12)70309-9. PMID: 19635247.) I point this out because I don’t believe science is close to duplicating the amazingly complex and rich oil found in healthy human tears - so I don’t find Castor Oil. (or any commercially available oil) to be a good substitute for the real thing!
From Eyes Are The Story, another link regarding eyelash growth serums containing Castor Oil: https://eyesarethestory.com/blogs/the-tome/eyelash-growth-serum-castor-oil-debunking-the-slippery-claims
To schedule an appointment with Dr. Jaccoma, call Excellent Vision at either of these two dry eye offices:
(1) 155 Griffin Rd, Portsmouth, NH 03801 (603) 574-2020
(2) 3 Woodland Rd, STE 112 Stoneham, MA 02180 (near Boston) (781) 321-6463
(July 23rd’s post includes an index to past posts which will not include this post but is otherwise a complete reference!)
Demodex – the tiny mite with a (sometimes) big effect on dry eye disease.

Demodex (& Seborrheic) Blepharitis
Demodex is a tiny mite that can be the stuff of nightmares – not because it is truly worthy of a nightmare for the great majority of us, but at least because it looks like a Sci-Fi creature from outer space. The problem is that it is a common part of our “inner space” and can contribute to the inflammation responsible for dry eyes and irritated eyelids.
When Biotissue brought Cliradex out as a weapon against Demodex, they quoted internal studies suggesting that the likelihood of acquiring Demodex is roughly 10 percent per decade – implying that by the time we are 100 years old, we are 100% likely to be carriers of Demodex (this now appears likely by the age of 70 – see below). Diagnosis then was typically based on seeing signs of blepharitis (inflammation and irritation of the eyelids) and then pulling out a number of eyelashes to examine the roots for living mites – using a high-powered microscope (100x).
Subsequent studies have shown that the presence of collarets (smallish, greasy collars of waste products produced by these mites that create a “turtleneck-like collar” around the base of the lashes) is diagnostic of mite infestation – so most clinicians no longer rely on the older method to confirm that a patient has these mites. Using this method, it is estimated that as many as 58% of an eye doctor’s patient base can be affected – so my perception is that it is much more common than previously thought.
There are problems with general demographic studies like this. The first is that Demodex is not always a problem. There are many patients who have evidence of substantial colonization with this mite – yet have no evidence of damage or associated irritation. Second, and what is most obvious - is that if you have it – you have it (regardless of your age) and if it is causing problems (which it doesn’t always do), then we need to “fix the problem.”
You might ask, apart from a careful eye exam by a dry eye specialist, how would one feel or otherwise know if they might have DB – otherwise known as “Demodex Blepharitis?” In reports by Yeu et al (Yeu E, Holdbrook M, Baba S, Gomes PJ. Psychosocial impact of Demodex blepharitis. Presented at: ARVO 2021. Abstract 3544849) and Schacter et al (Schachter S, Yeu E, Holdbrook M, Baba S, Gomes PJ. Clinical manifestations of Demodex blepharitis. Presented at: ARVO 2021. Abstract 3546575) it was reported that as many as 80% of affected patients had some symptoms related to DB. This was mostly noted as “eye irritation” for 4 years or more prior to diagnosis. Redness of the lids and difficulty wearing makeup or contact lenses as well as functional issues such as difficulty with nighttime driving were also common complaints. Dry eye specialists find it to be a common cause for loss of eyelashes and as a co-contributor to dry eye disease (largely based on the inflammation caused by the irritation – that hurts tear producing cells and glands).
A drug company named Tarsus has found that a common veterinary product used to treat mange and mites in animals (0.25% LOTILANER ophthalmic solution), happens to be a good treatment for DB in humans and is calling it XDEMVY. They also sponsored an informational, nation-wide program to help eye specialists identify DB - and are calling it “Look at the lids.” Since the collaret formation is diagnostic, the trick is for doctors to pay attention to this area of the lashes – and fortunately, having a patient “look down” (while examining with the office microscope - called a slit lamp) - makes it easy for the doctor to make the diagnosis.
XDEMVY has been FDA approved for this indication, but the company predicts it may not be nationally available in pharmacies until the end of this month. From the company information relating to the clinical studies that found safety and efficacy, they note:
“About XDEMVY™
XDEMVY (lotilaner ophthalmic solution) 0.25%, formerly known as TP-03, is a novel prescription eye drop designed to treat Demodex blepharitis by targeting and eradicating the root cause of the disease – Demodex mite infestation. The active ingredient in XDEMVY is lotilaner, which is a well-characterized agent that eradicates Demodex mites by selectively inhibiting the mite’s GABA-Cl channels. It is a highly lipophilic molecule, which may promote its uptake in the oily sebum of the eye lash follicles where the mites reside. XDEMVY was evaluated in two pivotal trials collectively involving more than 800 patients. Both trials met the primary endpoint and all secondary endpoints, with statistical significance and no serious treatment-related adverse events. Most patients found the XDEMVY eye drop to be neutral to very comfortable. The most common ocular adverse reactions observed in the studies were instillation site stinging and burning which was reported in 10% of patients. Other ocular adverse reactions reported by less than 2% of patients were chalazion/hordeolum (stye) and punctate keratitis.”
Other drug treatments targeted for Demodex include various strengths and forms of TTO (Tea Tree Oil, and its related compounds, including Cliradex) available over the counter, as well as various prescriptive strengths and forms of Ivermectin (topical creams being the most common). The recommended discussion points eye doctors have been advised to use in discussing this common problem is cited here (From: https://eyesoneyecare.com/resources/co-morbid-systemic-disease-that-complicates-osd/?utm_medium=eoe:infinite-scroll):
“Example patient education script for Demodex blepharitis
“Demodex are small mites that live on our skin, specifically in our hair follicles and oil glands. It is completely normal for these mites to be there, as we will all have them at some point in our lives, and, normally, they do not cause any issues. However, in some cases, the number of mites present gets too high, which leads to a buildup of their waste on our eyelids and eyelashes which causes irritation and redness. They can also clog up our oil glands which can cause styes to form.
Because these mites are not a bacterium or virus they cannot be treated with antibiotic or antiviral medication, so this makes them a little more difficult to treat.
The treatment that does work on the mites is tea tree oil which comes from the tea tree plant. This oil is very strong so it can be irritating to the eyes when you use it, but a strong treatment is needed because the mites can be very difficult to get rid of. When you apply the oil make sure to get it on the lids and lashes, especially near the margin of your lids because that is where the mites live. Try to avoid getting any of the oil in the eye itself because you will feel a stinging sensation if you do, this will not damage your eye, but it will be uncomfortable for a little while.
Also make sure to use the oil on your cheeks, nose, forehead, and eyebrows because the mites can live in these areas as well. We cannot get rid of all the mites even with tea tree oil treatment, so our goal is to bring down the number of mites to the point where they no longer cause any issues. The mites do come back in some cases, so you may have to use the tea tree oil long-term if needed, but you may not have to use it as often.”
My personal preference in treating these mites when they arise to the level of causing inflammation and aggravating eyelids and dry eyes, is as follows:
First, I generally don’t start with Demodex-specific treatment unless it is clear there is an abundant load or unless other avenues of common lid hygiene have failed to reduce the blepharitis and related inflammation. This is in part related to the fact that most general lid hygiene strategies can effectively reduce the Demodex load and because total eradication is unlikely, regardless of the methods used. I also believe that introducing a problem to a patient that has no guaranteed cure and which may not actually be a problem at all for many, is setting the patient up for anxiety and failure. I will have an honest and often lengthy discussion for those who insist on debating these issues, but when I believe it is necessary, I recommend the following protocol:
- Begin with good lid hygiene. I’ve covered this in posts before. Since stagnant oil is the “buffet table” for bacteria and since bacteria and stagnant oil is the foodstuff of the mites, then clearing off the greater percentage of bacteria will “starve” the mites and getting god flow of oil will reduce the stagnation that leads to the buffet table.
- Second, treat the collars and “plaque” with a BlephEx treatment. I’ve posted on this before (and find the eyeThera shields particularly good for ensuring an optimal level of clean for most of these treatments). This gets rid of the “footing” for these germs and mites and opens the door for deeper penetration of mite-specific treatments like TTO and Ivermectin (and soon, XDEMVY).
- Apply the TTO (or Cliradex) compounds to the lids, forehead, brows, cheeks, nose and chin. I find this is easiest with Cliradex foam or wipes, though when I prescribe 1% Ivermectin cream (available as the trade named “Soolantra” or as generic or compounded products), I instruct patients to rub a tiny pea-sized dose between the tips of the index fingers and then lightly massage it into the 4 eyelids – up to the lash line – but preferably not into the eyes, as it will sting but not damage the eyes. Then apply a ½ inch between the index and middle fingers of both hands and massage it into the forehead, brows, cheeks, nose and chin. Do this every night (the mites are more active at night and are more likely to come into contact with these products then) and continue for 4-6 weeks (depending on the load of Demodex I see and the effect it appears to be having on the lids and eyes).
- During this treatment time, consider treating anyone else who sleeps in the same bed, the same way, as they are often also carrying the same mites (even if they have no symptoms) and can serve as a reservoir for re-infestation. Also wash all bed sheets, pillowcases, towels, facecloths, and other products that come in regular contact with the face, as they can serve as reservoirs, too.
- IPL with a heated expression (I like the off-label use of RF I’ve described) is a good, non-drug-related avenue for clearing up Demodex and other causes of blepharitis. The IPL can help knock off some of the mites and germs, reduce the inflammation (by also closing off some of the inflammation-bearing blood vessels) and stimulate the glands making tears just as the heated expressions can turn over the stagnant oils (and likely purge the glands of the mites and germs otherwise occupying them). Adding oral or topical antibiotics can also help in select cases, as can topical anti-inflammatory medications.
- An exam within a month or so of completion can help to judge if the treatment was effective. If significant amounts of mites remain or rebound, then retreatment is often necessary – but remember that total eradication is not often possible, so seeing a much-diminished number of collarets and less redness of the lids is often an effective endpoint.
- Since not all blepharitis is Demodex-related, it is generally necessary to continue daily, basic lid hygiene forever – and in cases of frequent re-infestation, adding a TTO product to daily care is sometimes advisable. Other blepharitis can include fungal and allergic/allergen-related causes, so working with a good dry eye specialist can be crucial to good care.
To schedule an appointment with Dr. Jaccoma, call Excellent Vision at either of these two dry eye offices:
(1) 155 Griffin Rd, Portsmouth, NH 03801 (603) 574-2020
(2) 3 Woodland Rd, STE 112 Stoneham, MA 02180 (near Boston) (781) 321-6463
(July 23rd’s post includes an index to past posts which will not include this post but is otherwise a complete reference!)
Vitamin A – how important is it in treating – or causing – dry eye?
Vitamin A – how important is it in treating – or causing – dry eye?
As a senior resident in Ophthalmology, I was tasked to oversee the junior residents in their daily clinic. One day a bright junior resident approached me with the case of what was subsequently dubbed, “the peanut kid.” As this was close to 4-decades ago, the details should be hazy – but the important pieces remain clear as it was a true glimpse into a severe vitamin A deficiency the likes of which would rarely be seen outside of a third world country.
This approximately 13-year-old child had been seen by several city-wide eye doctors with the complaint of severely dry and irritated eyes. He’d been prescribed a variety of steroid and combination steroid and antibiotic eye drops, ointments, and artificial tears without relief. By the time he got to the resident’s clinic, his mother was upset and fortunately remained tirelessly committed to getting her son appropriate treatment. At the time of exam, he had “glassy eyes” that were glazing over with a roughened corneal surface, including some dry, triangular patches on the outer part of the eyeball (what this resident recognized as “Bitot Spots”).
Astutely, this resident asked the mother if there was anything unusual about her son’s diet. The amazing answer was something like this – “You’re the first doctor to ask about his diet and I’ve been reluctant to bring this up, but yes – he is quite unusual in that he only seems to like peanuts.” Subsequent inquiry determined that he would eat a bag of peanuts for breakfast, another for lunch and then two for supper. He would have “Hi-C” – an orange flavored drink rich in vitamin C, with breakfast and sometimes have ice cream after supper. These foods would provide the vitamins C and D along with calcium in the ice cream – and peanuts are a surprisingly good source of other vitamins, proteins, fats and minerals – so the remaining weak link in his dietary chain (apart from some essential Omega Oils) was Vitamin A.
Of further interest was the mother’s recall that as a younger child, when he first developed this peculiar interest in a peanut diet, his pediatrician told her that it would be a passing phase, and that she could keep him on a healthy track by supplying a (then Flintstones brand) child’s daily vitamin. At some point, around the time his pediatrician passed away, he stopped taking the vitamins and the new pediatrician seemed disinterested in her child’s diet. His health otherwise appeared “normal” so the idea this would be a passing phase caused her to go along with her son’s peculiar diet.
Further testing revealed he was almost totally night blind (an expected side effect of Vitamin A deficiency, as this vitamin is critical in supplying the retinal pigments responsible for vision in general – though night vision is typically the first to notably suffer). Lab work revealed an essentially undetectable level of Vitamin A in his bloodstream. The good news was that he responded quickly to vitamin A supplements, recovering his night vision, and restoring a healthy ocular surface.
Much research has been done in determining the benefits of Vitamin A in ocular health in general and in dry eye disease, in particular. My general sense is that short of an exceptional diet like the “peanut kid,” it is unlikely we will find many patients truly deficient in Vitamin A in the developed world – but as children get increasingly “picky” (and appear to subsist on diets based on pastries, chicken nuggets, mac and cheese and the like) – I find many who are deficient in essential Omega Oils (& believe a vitamin deficiency is not impossible).
I recently posted on Vitamin A products being touted for dry eye patients, thanks to the brilliant response by Dr. Peter Pham. I’ll paste that conversation here for those who want a deeper dive:
I’ll post her question and the excellent answer from Dr. Peter Pham (a chemist and ophthalmologist who invented the Zocuwipe and Zocugel products):
“Can someone please explain which forms of vitamin A are safe for meibomian glands…? I’m intrigued by the iVizia wipes and HyloNight ung, but hesitate to recommend after years of discouraging use of retinol on lids… any insight is greatly appreciated - thank you! “
Peter Pham: “Agree, am confused about retinoids myself. Such a complex topic with numerous patents and PhDs awarded on this topic, but the general rules of chemistry still apply. We shouldn't look at just one ingredient to determine whether a product is "safe" or "unsafe". This is especially true for "retinol", which comes in many forms. The most biologically active form is the carboxylic acid form, retinoic acid, which is two oxidation steps from the alcohol "retinol" form. Retinoids have multiple unsaturated isoprene chains and are inherently unstable. Just because a product has 1% or 0.1% retinol does not mean there's actually that much available since multiple other variables are involved from co-ingredients to packaging (airless bottles better than jars) to pH to temperature storage/fluctuations. If a retinol product is stored or transported at high temperatures or exposed to light, there may little useful retinol left, no matter what the initial percentage was. If a product is mostly water without much oil or emulsifiers, it's unlikely to be able to dissolve much retinol, which is oil soluble and we can predict that the percentage of retinol would be low. iVizia and Hylo both use the more stable ester form of retinol but what's not apparent from the ingredient list is that even the ester form needs to be stabilized, usually with the antioxidants butylated hydroxytoluene (BHT) or butylated hydroxyanisole (BHA) in the source product. There's an endless stream of superficial, fear-mongering posts about how BHT and BHA are "dirty" ingredients, with "retinols" mixed in there. But the mere presence of an ingredient does not make anything unhealthy or dirty. If a chemical is serving a useful purpose, it's unlikely to cause harm. Retinol helps to maintain ocular health - we know what happens when we lack it. And there's no doubt high doses of oral retinoic derivatives over a prolonged period can kill meibomian glands. As with everything, too much or too little of anything is never good.”
I’m not sure I know either. It does seem to vary by each case and may depend on the product and how it’s applied. Best to consult your dry eye specialist to get the best answer. Orally, eating plenty of leafy greens and colorful vegetables is the best source, as your body will convert these lutein and xeazanthein nutrients into active forms of Vitamin A as your body needs them. Too much active A can damage your liver, so unless you’re diagnosed as low, you generally don’t want to take the active form of Vitamin A in high quantities. Topically, your specialist can monitor the health of your eyes on appropriate supplements if they feel they are necessary.
To schedule an appointment with Dr. Jaccoma, call Excellent Vision at either of these two dry eye offices:
(1) 155 Griffin Rd, Portsmouth, NH 03801 (603) 574-2020
(2) 3 Woodland Rd, STE 112 Stoneham, MA 02180 (near Boston) (781) 321-6463
(Last week’s post includes an index to past posts which will not include this post but is otherwise a complete reference!)
Index of Blog Posts
This has been a labor of love - clipping and pasting all of the posts - with their links - from day 1.
Looks like I have written a bunch about dry eyes! I promise I won’t stop here - but thought I’d provide this Index, as many (rightly) get bogged down searching for an appropriate article or particular post when shuffling through the many that don’t relate.
For anyone “new” to my posts - I always suggest starting from the beginning (I lay the groundwork for subsequent posts this way) - and for anyone already caught up on all of my posts - I apologize that there is nothing “new” here today.
To schedule an appointment with Dr. Jaccoma, call Excellent Vision at either of these two dry eye offices:
(1) 155 Griffin Rd, Portsmouth, NH 03801 (603) 574-2020
(2) 3 Woodland Rd, STE 112 Stoneham, MA 02180 (near Boston) (781) 321-6463
More About Dry Eye and Glaucoma (spotlight on Durysta)
Jul 16
Written By Dr. Edward Jaccoma, MD
https://www.eyethera.com/blog/jwk8lv0558b5ewcp7cxummr7pusblv
The “Hill of Sorrow” and how getting better can sometimes feel like getting worse…
Jul 9
Written By Dr. Edward Jaccoma, MD
Can I use eye “whiteners” (like Visine or Lumify) when my eyes get red?
Jul 2
Written By Dr. Edward Jaccoma, MD
https://www.eyethera.com/blog/can-i-use-eye-whiteners-like-visine-or-lumify-when-my-eyes-get-red
What else is new? - A new numbing drop (& how it can help with things like Maskin Probing) and a new “implantable” steroid!
Jun 25
Written By Dr. Edward Jaccoma, MD
Are there any new eye drops for dry eye?
(Miebo and Reproxalap)
Jun 18
Written By Dr. Edward Jaccoma, MD
https://www.eyethera.com/blog/are-there-any-new-eye-drops-for-dry-eye
Do results of IPL treatment vary by technique and by the filters used? (& does it regenerate withered glands?)
Jun 11
Written By Dr. Edward Jaccoma, MD
Manuka Honey - How sweet it is (or might be?) for treating dry eyes!
Jun 4
Written By Dr. Edward Jaccoma, MD
https://www.eyethera.com/blog/manuka-honey-how-sweet-it-is-or-might-be-for-treating-dry-eyes
Can eye drops kill you? Part 2: avoiding “Buyer’s Remorse.”
May 28
Written By Dr. Edward Jaccoma, MD
https://www.eyethera.com/blog/can-eye-drops-kill-you-part-2
Can eye drops kill you? Part 1:
May 21
Written By Dr. Edward Jaccoma, MD
https://www.eyethera.com/blog/can-eye-drops-kill-you-part-1
Do Eye Drops Cause Ringing In The Ears & Can Ringing In The Ears Mean Eye Problems?
May 14
Written By Dr. Edward Jaccoma, MD
When tears don’t drain properly you get “Toxic Soup.” (and the “Toxic Soup Syndrome!”)
May 7
Written By Dr. Edward Jaccoma, MD
Common Eyelid problems related to dry eye disease:
Part 6b: When tears run over the eyelids (visibly crying when you don’t mean to, Part 2)
Apr 30
Written By Dr. Edward Jaccoma, MD
https://www.eyethera.com/blog/5ud2bzqqq5iu88dsoh6wnnbgws0fze
Common Eyelid problems related to dry eye disease: Part 6a: When tears run over the eyelids (visibly crying when you don’t mean to, Part 1 of 2)
Apr 23
Written By Dr. Edward Jaccoma, MD
https://www.eyethera.com/blog/zmhihjvx9qfdibtgi1f2ppmkfj9fdr
Common Eyelid problems related to dry eye disease, Part 5: Floppy Eyelids!
Apr 16
Written By Dr. Edward Jaccoma, MD
Common eyelid problems related to dry eye disease, Part 4: The eyelid “innie.”
Apr 9
Written By Dr. Edward Jaccoma, MD
Part 4: When eyelids turn in the wrong direction: Entropion = turns in
Common Eyelid problems related to dry eye disease, Part 3: The eyelid “outtie.”
Apr 2
Written By Dr. Edward Jaccoma, MD
Part 3: When eyelids turn in the wrong direction: Ectropion = turns out
https://www.eyethera.com/blog/common-eyelid-problems-related-to-dry-eye-disease-part-3-ectropion
Common eyelid problems that can relate to dry eye disease, Part 2: Say Hi to “TED.” (Thyroid Eye Disease)
Mar 26
Written By Dr. Edward Jaccoma, MD
https://www.eyethera.com/blog/8lemgnwt0bqqd15fmqr9ljrkdfe420
Common eyelid problems that can relate to dry eye disease, Part 1: Bad lashes.
Mar 19
Written By Dr. Edward Jaccoma, MD
https://www.eyethera.com/blog/0r1w3kiho48uaz4yydxlyrogx5xksf
What about Punctal Plugs (or - “Why not dam up those tears”)?
Mar 12
Written By Dr. Edward Jaccoma, MD
https://www.eyethera.com/blog/what-about-punctal-plugs-or-why-not-dam-up-those-damn-tears
What happens when you don’t have enough good oil and how do you fix it? (SLK, CCH and why blinking matters)…
Mar 5
Written By Dr. Edward Jaccoma, MD
Sjogren’s Disease: Autoimmune dry eye Part 5
Feb 26
Written By Dr. Edward Jaccoma, MD
https://www.eyethera.com/blog/ogh4ia5gewpejt9cszlk0emeccuzh3
Sjogren’s Disease: Autoimmune dry eye Part 4
Feb 19
Written By Dr. Edward Jaccoma, MD
https://www.eyethera.com/blog/lii4sjra1r8e55qofjooka84ccyclr
Sjogren’s Disease: Autoimmune dry eye Part 3
Feb 12
Written By Dr. Edward Jaccoma, MD
https://www.eyethera.com/blog/sjogrens-disease-autoimmune-dry-eye-part-3
Sjogren’s Disease: Autoimmune dry eye Part 2
Feb 5
Written By Dr. Edward Jaccoma, MD
https://www.eyethera.com/blog/sjogrens-disease-autoimmune-dry-eye-part-2
Sjogren’s Disease: Autoimmune dry eye Part 1
Jan 29
Written By Dr. Edward Jaccoma, MD
https://www.eyethera.com/blog/sjogrens-disease-autoimmune-dry-eye-part-1
This is #52 of my Dry Eye Posts!
Jan 22
Written By Dr. Edward Jaccoma, MD
https://www.eyethera.com/blog/521429-weeks-in-a-year-and-this-is-52-of-my-dry-eye-posts
Do blue blocking glasses help with dry eyes?
Jan 15
Written By Dr. Edward Jaccoma, MD
https://www.eyethera.com/blog/do-blue-blocking-glasses-help-with-dry-eyes
More on MGs (the tear oil glands)
Jan 8
Written By Dr. Edward Jaccoma, MD
https://www.eyethera.com/blog/more-on-mgs-the-tear-oil-glands
How Safe and Effective are Home-Based Radiofrequency and Light Treatments for Dry Eye Care?
Jan 1
Written By Dr. Edward Jaccoma, MD
Why do some people produce “pasty meibum?” PART 4
Dec 18
Written By Dr. Edward Jaccoma, MD
https://www.eyethera.com/blog/why-do-some-people-produce-pasty-meibum-part-4
Why do some people produce “pasty meibum?” PART 3
Dec 11
Written By Dr. Edward Jaccoma, MD
Why do some people produce “pasty meibum?” PART 2
Dec 4
Written By Dr. Edward Jaccoma, MD
https://www.eyethera.com/blog/why-do-some-people-produce-pasty-meibum-part-2
Why do some people produce “pasty meibum?” (Part 1)
Nov 27
Written By Dr. Edward Jaccoma, MD
https://www.eyethera.com/blog/why-do-some-people-produce-pasty-meibum
Doctor, I have a bright red spot on my eye! What (else) do I do now (about a subconjunctival hemorrhage, Part 2)?
Nov 20
Written By Dr. Edward Jaccoma, MD
https://www.eyethera.com/blog/cdyemollbn8blvmic6jqtg7i8yipx8
Doctor, I have a bright red spot on my eye! What caused it, is it dangerous and what do I do now (about a subconjunctival hemorrhage, Part 1)?
Nov 13
Written By Dr. Edward Jaccoma, MD
Problems with use and proper care of a Bruder (or similar) moist heat eyelid mask.
Nov 6
Written By Dr. Edward Jaccoma, MD
https://www.eyethera.com/blog/proper-use-and-care-of-a-bruder-or-similar-moist-heat-eyelid-mask
How do everyday products affect our eyes?
Oct 30
Written By Dr. Edward Jaccoma, MD
https://www.eyethera.com/blog/how-do-everyday-products-affect-our-eyes
What’s new in treating Blepharitis?
Oct 23
Written By Dr. Edward Jaccoma, MD
https://www.eyethera.com/blog/whats-new-in-treating-blepharitis
My IPL Demo and “Pearls” for optimal treatment.
Oct 16
Written By Dr. Edward Jaccoma, MD
https://www.eyethera.com/blog/my-ipl-demo
What makes “enough,” ENOUGH and is there such a thing as “too much?” PART 3
Oct 9
Written By Dr. Edward Jaccoma, MD
https://www.eyethera.com/blog/what-makes-enough-enough-and-is-there-such-a-thing-as-too-much-part-3
What makes “enough,” ENOUGH and is there such a thing as “too much?” PART 2
Sep 25
Written By Dr. Edward Jaccoma, MD
https://www.eyethera.com/blog/what-makes-enough-enough-and-is-there-such-a-thing-as-too-much-part-2
What makes “enough,” ENOUGH and is there such a thing as “too much?” (Part 1)
Sep 18
Written By Dr. Edward Jaccoma, MD
https://www.eyethera.com/blog/what-makes-enough-enough-and-is-there-such-a-thing-as-too-much
What can a good first step in lid hygiene look like?
Sep 11
Written By Dr. Edward Jaccoma, MD
https://www.eyethera.com/blog/what-can-a-good-first-step-in-lid-hygiene-look-like
“I’ve tried everything - now what?”
Aug 28
Written By Dr. Edward Jaccoma, MD
https://www.eyethera.com/blog/ive-tried-everything-now-what
The “2-Ps” - Pingecula and Pterygium - and Dry Eye Disease…
Aug 22
Written By Dr. Edward Jaccoma, MD
https://www.eyethera.com/blog/the-2-ps-pingecula-and-pterygium-and-dry-eye-disease
Special cases for healing the eye’s surface - Part 2: Map-Dot-Fingerprint Corneal Dystrophy (MDF).
Aug 14
Written By Dr. Edward Jaccoma, MD
https://www.eyethera.com/blog/5b9vbda1r8e8r5y07l9bslgttcl4d8
Special cases for healing the eye’s surface - Part 1: Recurrent Corneal Erosions (RCE).
Aug 7
Written By Dr. Edward Jaccoma, MD
What to do when the surface of your eye gets “broken” (scratched, operated on, infected or otherwise damaged).
Jul 31
Written By Dr. Edward Jaccoma, MD
Avoiding a “Heart Attack” on the surface of your eye…
Jul 24
Written By Dr. Edward Jaccoma, MD
https://www.eyethera.com/blog/avoiding-a-heart-attack-on-the-surface-of-your-eye
The Ocular “Heart Attack” of a Stare. (And why digital devices can cause these “heart attacks.”)
Jul 17
Written By Dr. Edward Jaccoma, MD
Do you have “Mom’s” (or Dad’s) eyes?
Jul 10
Written By Dr. Edward Jaccoma, MD
https://www.eyethera.com/blog/do-you-have-moms-or-dads-eyes
Why do expensive dry eye treatments fail? (And what is Maskin Probing?)
Jul 4
Written By Dr. Edward Jaccoma, MD
https://www.eyethera.com/blog/why-do-expensive-dry-eye-treatments-fail-and-what-is-maskin-probing
What is “Neurostimulation” for dry eye treatment and do I need it?
Jun 26
Written By Dr. Edward Jaccoma, MD
https://www.eyethera.com/blog/what-is-neurostimulation-for-dry-eye-treatment-and-do-i-need-it
More on IPL:
Jun 19
Written By Dr. Edward Jaccoma, MD
https://www.eyethera.com/blog/more-on-ipl
CCH part 3: When do we treat CCH – and what are the non-surgical options?
Jun 12
Written By Dr. Edward Jaccoma, MD
https://www.eyethera.com/blog/cch-part-3-when-do-we-treat-cch-and-what-are-the-options
Conjunctival Chalasis (CCH) part 2 - How do we fix it?
Jun 5
Written By Dr. Edward Jaccoma, MD
https://www.eyethera.com/blog/conjunctival-chalasis-cch-part-2-how-do-we-fix-it
What is Conjunctival Chalasis (CCH) and why should I care?
May 29
Written By Dr. Edward Jaccoma, MD
https://www.eyethera.com/blog/what-is-conjunctival-chalasis-cch-and-why-should-i-care
When eyelids are irritated (including “mucus fishing” - as well as allergies, such as to our best friend - pets!)
May 22
Written By Dr. Edward Jaccoma, MD
Why did I get a stye (Chalazion)?
May 15
Written By Dr. Edward Jaccoma, MD
https://www.eyethera.com/blog/why-did-i-get-a-stye-chalazion
Contact lenses and dry eye - Part 2
May 8
Written By Dr. Edward Jaccoma, MD
https://www.eyethera.com/blog/6g9blza7q7q9zmhychmq509nsad9a4
Contact lenses and dry eye - Part 1
May 5
Written By Dr. Edward Jaccoma, MD
https://www.eyethera.com/blog/z9r2sgjxe1iyza1k6535laildtqilm
“Why do my oil supplements not work?
Apr 24
Written By Dr. Edward Jaccoma, MD
https://www.eyethera.com/blog/why-do-my-oil-supplements-not-work
Dry eye: Cataract and Glaucoma Segment
Apr 17
Written By Dr. Edward Jaccoma, MD
https://www.eyethera.com/blog/dry-eye-cataract-and-glaucoma-segment
Segment 12. IPL for dry eye - common concerns and questions
Apr 10
Written By Dr. Edward Jaccoma, MD
https://www.eyethera.com/blog/lwbovaedc1wjw2rrhvp0qosg2m9858
Why can’t I just use some tear drops or ointments instead of all this work?
Apr 3
Written By Dr. Edward Jaccoma, MD
(not so) Secret Weapon of Dry Eye Treatment: Intense Pulsed Light, or IPL
Mar 27
Written By Dr. Edward Jaccoma, MD
https://www.eyethera.com/blog/not-so-secret-weapon-of-dry-eye-treatment-intense-pulsed-light-or-ipl
Segment 10 B - When we are at war with ourselves.
Mar 20
Written By Dr. Edward Jaccoma, MD
https://www.eyethera.com/blog/segment-10-b-when-we-are-at-war-with-ourselves
Segment 10 A - What we know about inflammation…
Mar 13
Written By Dr. Edward Jaccoma, MD
https://www.eyethera.com/blog/segment-10-aampb-what-we-know-about-inflammation
More on Germs
Feb 28
Written By Dr. Edward Jaccoma, MD
https://www.eyethera.com/blog/more-on-germs
Dealing With Germs
Feb 20
Written By Dr. Edward Jaccoma, MD
https://www.eyethera.com/blog/dealing-with-germs
“You Are What You Eat”
Feb 13
Written By Dr. Edward Jaccoma, MD
https://www.eyethera.com/blog/you-are-what-you-eat
How Do We Fix The Oil Problem?
Feb 6
Written By Dr. Edward Jaccoma, MD
https://www.eyethera.com/blog/how-do-we-fix-the-oil-problem
How Do We Know If We Have Dry Eye Disease? (see also, Dr. Jaccoma’s simple, at home dry eye test, in his earlier post-link here: https://www.eyethera.com/blog/rn9p8ouyjzjhyfpkvrysxjx28no0q8 )
Jan 30
Written By Dr. Edward Jaccoma, MD
https://www.eyethera.com/blog/how-do-we-know-if-we-have-dry-eye-disease
How Important is Oil to Our Tears?
Jan 23
Written By Dr. Edward Jaccoma, MD
https://www.eyethera.com/blog/how-important-is-oil-to-our-tears
Overly Salty Tears
Jan 16
Written By Dr. Edward Jaccoma, MD
Segment 3 Too much salt in the salad dressing.
https://www.eyethera.com/blog/overly-salty-tears
Why Tears Are Important (& why should we even worry about our tears?)
Jan 5
Written By Dr. Edward Jaccoma, MD
https://www.eyethera.com/blog/why-tears-are-important
Introduction To Dry Eye Disease
Dec 29 (Take Dr. Jaccoma’s simple, at home “Dry Eye Test”)
Written By Dr. Edward Jaccoma, MD
https://www.eyethera.com/blog/rn9p8ouyjzjhyfpkvrysxjx28no0q8
More About Dry Eye and Glaucoma (spotlight on Durysta)
Dry eye and glaucoma - they often go together, hand in hand. Partly this may mirror the age groups affected (though younger ages are increasingly more affected by dry eye and less by glaucoma - it is also true that as we age, incidence of both will rise). I covered a general discussion of this earlier (see my earlier link and more information, below).
What is glaucoma? Technically, vision comes from the capture of light, conversion of that light to electrical energy, the transfer of that energy to our brain and the “unscrambling” of that electronic signal to form a mental image. Simply, it is easier to explain by thinking back to the pre-cable television era. Before cable TV, there were antennas that were perched on our rooftops - or else existed as “rabbit ears” on top of our TV sets. They would capture the signals beamed from TV stations and convert that energy into electricity that was delivered to the back of TV sets by wires covered in brown plastic insulation. The plastic was scrapped off so the copper wire strands would be wound around little screws in the back of the TV to make a connection. Those of us who lived through that time might recall a time when, no matter what you did with the “tuning” of the antenna (remember swiveling the “rabbit ears” or wrapping them in tinfoil?), and no matter what you did with the tuning dial on the TV set itself, you couldn’t get a clear picture (or sometimes any picture) until you realized that the wires of your antenna had frayed or come loose and you had to freshen up the connection to get a clear picture. That is the essence of glaucoma, except we can’t freshen that connection or reconnect what is lost - once the “wires” (which are really tiny cells) are lost - we can’t get them back. The poor picture will only get worse - until all of the wires (and picture) are gone. That is glaucoma - and that is why we must work to prevent that outcome.
The “problem” is that we are all born with about one million “wires” (or cell fibers) per eye - and we can lose 4,000-5,000/year just through “normal wear and tear.” That implies that if any of us live long enough, we could all die blind. In reality, this would mean we would have to live hundreds of years to lose all of our vision - and since none of us live that long (yet), we don’t generally have to worry about that. Glaucoma happens when these fibers “fray” or die-off faster than normal. This can occur from genetic causes (smaller, less substantial nerves or more fragile nerves), from trauma (head or eye injuries) or from the multitude of issues that can cause increased pressure inside the eye. What eye doctors have learned is that if we can lower eye pressure enough, we can slow down this loss of fibers and preserve the nerve’s function (though we can never completely stop the natural process of some loss - just slow it down enough that we can prevent people from dying blind or visually disabled from glaucoma). The bigger problem is that we are all living longer - so eye doctors feel a greater need to diagnose - and to more aggressively treat - glaucoma to save our patients from dying blind.
Eye pressure (known as “IntraOcular Pressure” or IOP) is the result of the difference of how much “water” is made in the eye and how much of this “water” can leave the eye - think plumbing. In our eyes we have living cells - and like every living cell in our bodies, these cells need support. Where most of our living cells get their support from blood, the cells inside the front of our eyes con’t have blood - so they have a clear, water-like solution called aqueous humor (and the cells on the outer surface of our eyes have tears) for support. Simply put, the cells take what they need to survive from this “water” (called aqueous humor) and then put their “waste” into it. This “dirty, used up water” then needs to leave our eye. It does so by way of a filtered drain. The “waste” (pigments, proteins and cellular debris) gets deposited into the cheesecloth-like filter and the pure water returns to our circulation. As quickly as this “water” is made, circulates, and does its job, it then needs to leave they eye. If the filter clogs or there is a relative blockage anywhere in the “plumbing system” then the water backs up and causes pressure - until that pressure overcomes the blockage so the water can leave.
As a dry eye specialist who also sees glaucoma patients, my general recommended protocol was communicated in my earlier blog post, here: https://www.eyethera.com/blog/dry-eye-cataract-and-glaucoma-segment I continue to advocate for SLT, Durysta and less preserved, IOP-reducing eye drops (including the combined products that can deliver two medications in one drop). My experience with the Durysta glaucoma medication implant has grown since then, and I find it can be a great tool for getting more medication off of the eye’s surface and into the eye (where it needs to be, in order to do the work needed by lowering IOP).
Of interest, is the way the so-called Prostaglandin Analogs (PGAs) like Durysta (as well as the topical versions such as Latanoprost, Travoprost and Bimatoprost) work. Using my analogies and a fundamental understanding of evolution, I surmise that back in our cave-people-origin days, if our eyes got whacked in hunting, gathering or defending our clan - the response to a damaged eye (and damaged internal drain) could be a loss of sight from the pressure backing up inside the eye as it healed. Poor vision (or no vision) could lead to less procreation and extinction. Evolution came up with a hormone-like chemical our bodies can manufacture (prostaglandins or PGs) which can open a “pressure-relief-valve” inside the eye, that can send the internal watery fluid around the clogged or damaged drain and into a “special drain” (so-called uveoscleral outflow, for those who want to be in the know). As the eye heals, it makes less of this prostaglandin (PG) compound. Scientists discovered a way to create chemicals that act like our own PGs (so called Prostaglandin Analogs or PGAs). When they find their way into the eye, they open the same “pressure relief valve” and drop IOP as long as we use the drop (or have the implant working).
Typical drop-forms of PGAs contain preservatives (intentionally toxic chemicals designed to prevent germs or green fuzzy stuff from growing in the dropper and then getting on our eyes) - but now those preservatives can damage the cells that make our tears - and damage the cells served by those tears - so there is a love-hate relationship with these preserved medications. Durysta (and some newer PGA drops) is/are preservative free. Any IOP controlling chemical added to the surface of our eye as a drop, is going to “wash away” whatever tear was there - and has to “sit” long enough on the surface, to penetrate into the eye and do its job in there. Durysta is placed (quickly and painlessly) inside the eye - so there is no competition with tears, nor any toxic effect on the surface (it sits inside and gradually dissolves. Once dissolved, it most often will keep the “pressure relief valve “stuck open” for some months before that valve gradually closes and another implant is needed). It is important to make sure a PGA is indicated for IOP control and that there is no PGA allergy or expected unwanted side effects (every medication can have some and it is up to the doctor who would place it, to also consider when and if to place it - and then counsel you to help you decide if it is right for you). Glaucoma can be a complicated disease to diagnose and to manage, (as is dry eye disease) so having an experienced doctor help you with those decisions is critical to getting the best help.
More information on Durysta can be found here: https://www.durysta.com/
To schedule an appointment with Dr. Jaccoma, call Excellent Vision at either of these two dry eye offices:
(1) 155 Griffin Rd, Portsmouth, NH 03801 (603) 574-2020
(2) 3 Woodland Rd, STE 112 Stoneham, MA 02180 (near Boston) (781) 321-6463
The “Hill of Sorrow” and how getting better can sometimes feel like getting worse…
As a dry eye specialist, I can attest that the symptoms of dry eye disease can be wildly variable from patient to patient. The scariest patients are the ones with advanced dry eye disease and related ocular surface diseases, who have little to no symptoms. This is most often related to the slow onset of this often insidious disease. I like the analogy of adding a daily single straw to a camel’s back. From one day to the next, the camel is largely unaware he (or she) is carrying any straw at all - until one day (perhaps from a small stumble - in this analogy - but now think of what a stumble could be to a dry eye - perhaps a little allergy, or minor infection, a surgery, a new glaucoma medication or just staring at a digital screen a little too long), now the camel falls down and can’t get up again. Even worse is when the corneal nerves that serve the surface become slowly damaged from a lack of healthy tears (or other diseases like diabetes or infections like shingles). Now, as the tears get worse and the surface gets drier and more damaged, the eyes actually start to feel “better” because they are getting numb from the damage. These patients may feel worse as we start to improve their tears, and heal their surface and nerves. This can explain why some patients are being told by their doctor that they are getting better even as they feel they are getting worse. Fortunately most will eventually feel better as they get better (this has been dubbed the “Hill of Sorrow” by Dr. White of Sky Vision). The short answer is that dry eye is a complex disease with an equally complex range of findings and symptoms. Best to find a good dry eye specialist and work closely with them until you get better - and then work even harder to stay that way. Caught early, it can be pretty simple to take care of, but caught late it can be a really tough road to fix.
To schedule an appointment with Dr. Jaccoma, call Excellent Vision at either of these two dry eye offices:
(1) 155 Griffin Rd, Portsmouth, NH 03801 (603) 574-2020
(2) 3 Woodland Rd, STE 112 Stoneham, MA 02180 (near Boston) (781) 321-6463
Can I use eye “whiteners” (like Visine or Lumify) when my eyes get red?
As a dry eye specialist, I frequently get questions like this. The simplest answer is “rarely!” Redness is a sign of inflammation (from any of many causes). Inflammation is the body’s response to irritation and will dilate blood vessels so they can deliver larger quantities of the body’s natural defenses to the site of irritation (in this case, the eyes). Anything that make eyes look “whiter” (like regular Visine or the newer drop, Lumify) by causing the big, red blood vessels to constrict (“shrinking them”), will risk “rebound redness” when the little muscles in those blood vessels eventually need to “relax.” Most can get away with this if they’re only using it “once in a blue moon.” Doing this over and over, leads to “addiction,” where skipping the drop makes eyes red, swollen and miserable. The bigger problem is that the more you use the drop, the faster it wears off, requiring more frequent applications and giving less relief. (Think of the rebound issues for those who regularly use nasal decongestants like Afrin). Add to that - the fact that these drops contain preservatives (like BAK) that prevent green, fuzzy stuff from growing in the bottle. Preservatives are toxic chemicals able to kill germs, but also capable of harming tear glands, which can make you progressively more dependent on artificial tear products (since you no longer can make your own). For those already suffering from this addiction, the best recourse is to work with a dry eye specialist who can provide better treatments to address the root cause of the redness (like dry eyes, toxic makeup products, blepharitis and/or allergies) and will sometimes prescribe slow tapers with supportive anti-inflammatories (like low dose steroids) to assist in the recovery. I’ve posted a lot on tears and dry eye treatments. One is available here: https://www.eyethera.com/.../why-cant-i-just-use-some...